Author(s): Girish J Kotwal
There is little doubt due to abundant evidence that the multiple vaccines from Pfizer, Johnson and Johnson, AstraZeneca and Moderna against COVID and its emerging variants are safe and effective [1-4]. Every person who has never been infected with COVID and has not yet been fully immunized, should enthusiastically get fully immunized. There is very little evidence to conclusively suggest how vaccines protect even after, 161 million US residents have been fully immunized. The only way to determine what protects is to exhaustively study what has enabled 33+ million US residents and 186+ million worldwide to survive a whole range of mild to severe symptoms of COVID and acquire robust ADAPTIVE IMMUNITY in the process of completely clearing the infection. While vaccines simulate the acquisition of immunity, they do not provide deeper insights into what really protects. That is why I am advocating more studies of the components of the immune system that have successfully cleared the infection with broad adaptive natural immune response and greatly diminished the chances of reinfection for long periods. The answer to the question how long such a natural immunity will be protective against reinfection or infection caused by emerging variants before a vaccine booster dose may be required is key for public health. In order, to begin to dissect the natural antibody response to COVID just as it has been done for decades for Hepatitis B virus infection, LabCorp has recently introduced a test to detect antibodies to the most abundant protein of COVID, the nucleocapsid protein and to quantify antibody levels against COVID [5]. As an example, is a Final Lab. Report from LabCorp, of a person exposed to COVID around Nov. 03, 2020, confirmed positive on Nov. 12, 2020, has been COVID free since Dec. 12, 2020 and never been vaccinated against COVID (Table 1). The purpose of LabCorp was to be able to differentiate antibodies from a past infection among those who have not received the vaccine, from a vaccination and to quantify the duration of such an antibody response by a long term follow up. From a public health standpoint, establishing a standard of long-term care following COVID infection by regular monitoring of antibody levels and the breadth of the response would be ideal. Besides periodically evaluating immune status and detecting any COVID reinfection, survivors of COVID need to stringently be followed by a team of medical experts and certified therapists in Endocrinology, Urology, Internists, Infectious Diseases experts, Kidney care specialists, Pulmonology, Cardiology, Primary care, Psychiatry, Neurology, Podiatry, Rehabilitation Medicine. One in 3, COVID recovered persons could have brain dysfunction and long-term symptoms ranging from fatigue to Alzheimer’s Disease-like dementia or Tinnitus.
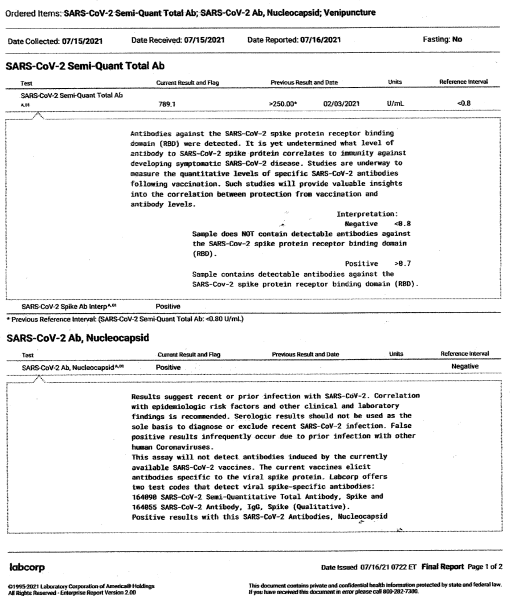
Table 1: Final Labcorp Report Covering Name and Address of the Patient
The author does NOT have any conflict of interest. Not affiliated to any political party in the USA or China.
The precise contribution of those acknowledged below is for input to the rigorous debate that was seriously considered in the intense deeper thinking of the sole author and by no means a consent or an agreement with all the contents or suggestions for consideration. Neither of those acknowledged nor the author had any role in the actual laboratory testing that generated the independent blind lab. report from a reputed diagnostic laboratory, Labcorp. The guidance for interpretation is clearly indicated in the report and the author does not conclude anything beyond the guidance for interpretation. A larger study of a vaccinated cohort and unvaccinated cohort of those who cleared the virus for several months following a diagnosis of viral infection is clearly recommended by the author using the approach outlined in the publication. Currently there is a large study of an estimated 4000 households underway in Louisville, KY, USA. The author had no role in the design of the Louisville, KY study, but does participate in this COVID immunity study as a subject who signed off on the informed consent form and has received periodic reports that were also taken into consideration to conclude that there was no reinfection noted during the 8 months following clearance of severe near death COVID infection that required ICU hospitalization and careful long term followup rehabilitation care. A large study by Gazit et al. from Israel has subsequently been published on August 25, 2021 in MedRxiv and can be found on the following link. This study clearly confirms that the natural immunity acquired by COVID warriors who had severe COVID infection and recovered have an immunity that is superior to those fully immunized against COVID.
https://www.medrxiv.org/content/10.1101/2021.08.24.2126241 5v1#disqus_thread
Dr. Bernard Moss, MD, Ph.D., NIH Distinguished Investigator, Laboratory of Viral Diseases, Genetic Engineering Section, National Institute of Allergy and Infectious Diseases (NIAID), Bethesda, MD, USA.
Prof. Sufan Chien, MD, Professor of Surgery, University of Louisville of Louisville School of Medicine and Founder and CEO of Noveratech LLC, Louisville, USA.
Assoc Prof. Stuart N. Isaacs, MD Perelman School of Medicine at the University of Pennsylvania, Division of Infectious Diseases, Department of Medicine, Philadelphia, PA USA.
Dr. Sanjai Nagendra, MD, MMM, CPE Medical Director Labcorp Center for Esoteric Testing and Atlantic Regional Laboratories, Raleigh-Durham-Chapel Hill Area, NC, USA.
Prof. Dr. Gerd Sutter, Project Coordinator Ludwig-MaximiliansUniversitat Munchen, Germany
Prof. Rachael Roper, Professor, Department of Microbiology and Immunology, Eastern Carolina University, Greenville, NC, USA.
Dr. Svarit Dave, M.D., family medicine physician at Norton Community Medical Associates Brownsboro. Dr. Dave is member of American Academy of Family Physicians, the Kentucky Academy of Family Physicians, the American Medical Association and the Kentucky Medical Association. He is board certified in family medicine.
Prof. Douglas Golenbock, M.D. The Neil and Margery Blacklow Chair in Infectious Diseases and Immunology Professor and Chief, Division of Infectious Dis.and Immunology, Dept of Med. UMass Med. School, Worcester, MA, USA.
Prof. Sanjay Ram, MD, Division of Infection Diseases, Department of Medicine, UMass Memorial Medical Center Worcester, Massachusetts, USA.
Prof. Peter Rice, MD, Division of Infectious Diseases, Professor of Medicine at UMass Medical School, Worcester, Massachusetts, USA.
Prof. Geoffrey Lilley Smith Ph.D. FRS FMedSci FRSB Professor of Virology and Head of the Department of Pathology at the University of Cambridge and a Principal Research Fellow of the Wellcome Trust, UK.
Dr. Subbian Sathesh Panayampalli Lead, Immunodiagnostic team and Poxvirus and Rabies branch, Centers for Disease Control (CDC) Atlanta, Georgia, USA.
Prof. Grant McFadden , Director, Center for Immunotherapy, Vaccines and Virotherapy (B-CIVV), Biodesign Institute, Arizona State University Tempe, AZ, USA
Prof. Sri Prakash L. Mokshagundum, M.D., Professor of Medicine, Chief Division of Endocrinology, Metabolism & Diabetes, University of Louisville School of Medicine and Chief of Endocrinology, Robley Rex Veterans Affairs Medical Center, UoFL Physicians Outpatient Center, Louisville, KY, USA.
The Lab testing cost was covered by Medicare of the USA. Medicare is a national health insurance program in the US, begun in 1965 under the Social Security Admin and now administered by the Centers for Medicare and Medicaid Services in the Department of Health and Human Services (DHHS), US govt.
Delaying vaccination by individuals who were naturally infected with SARS-CoV-2 in order to follow antibody levels does not reflect the opinion of Dr. Bernard Moss or to my knowledge that of the National Institute of Allergy and Infectious Diseases (NIAID, NIH).