Author(s): Nkem Obiechina* and Ahmad Soolari
A number of changes occur in the alveolar ridge following tooth extraction such as remodeling of bone in the alveolar ridge that can lead to loss of alveolar ridge width and height. Studies have shown that most of the changes occur in the first three months following teeth extraction. The goal of alveolar ridge preservation procedures is to maintain the dimensions of the extraction site, reduce significant loss of alveolar ridge and height and maintain adequate bone for dental implant placement. Alveolar ridge preservation also helps prevent the need for additional procedures prior to dental implants such as utilization of block grafting for ridge augmentation and sinus augmentation. It is indicated for both intact extraction sockets and extraction sites with significant damage to its walls. The goal of this article is to present two case reports on patient management for extraction sockets with damaged boney walls using Alveolar ridge preservation.
Following extraction of a tooth, a number of changes occur in the alveolar ridge involving modelling and remodeling of bone resulting in a significant loss of bone in horizontal and vertical dimensions of the ridge within the first year following tooth extraction without immediate implant placement. According to Schropp and colleagues most of these dimensional changes occur within the first three months following tooth extraction [1]. In their study using subtraction radiography to assess changes in extraction sockets over a 12-month period, 50% of the width of the alveolar ridge was reduced with the loss corresponding to a 5-7mm in width [1]. The greatest loss of ridge width occurred in the first three months.
Immediate Implant placement in fresh extraction sockets is a successful protocol for preserving alveolar ridge dimensions and has been recommended as the treatment of choice when feasible. For a number of reasons such as the presence of bone defects, potential for esthetic compromise, proximity to vital structures and failure to achieve implant stability, immediate implant might not be an option [2].
Placement of implants at a later time after healing of the extraction socket becomes necessary. When no ridge preservation occurs in the extraction site, significant dimensional changes can occur in the site resulting in loss of alveolar ridge width and height.
Bone loss after tooth extraction causes two major challenges, esthetic problems around fixed dental prosthesis resulting in soft tissue recession or it can make dental implant placement more challenging with a need for guided bone regeneration to be performed [2]. Alveolar ridge preservation is defined as any local therapeutic intervention performed at time of tooth extraction primarily aimed at preserving alveolar ridge contours in order to have maximum bone and soft tissue available for future implant placement or delivery of tooth supported prosthesis [3].
Alveolar ridge preservation techniques can be utilized for intact sockets with the intention of retaining the dimensions of the socket, this is called socket preservation, or it can be utilized for damaged extraction sockets that present with severe dehiscence or fenestration defects which are defined as defects involving a minimum of 50% of alveolar height of any socket wall [3].
To address bone loss and preserve the dimensions of the alveolar ridge, ridge preservation techniques are treatment planned with tooth extraction with the goal of maintaining the contours of the alveolar ridge, and preserving the bone in the extraction site to allow placement of dental implants and fixed restorations. Alveolar ridge preservation is effective in limiting physiologic ridge reduction compared to tooth extraction alone.3A number of studies have been able to show the proven effect of Alveolar ridge preservation procedures on maintaining alveolar ridge dimensions and minimizing loss of tissue volume [2-6].
Factors that affect effectiveness of alveolar ridge preservation procedures include number of neighboring teeth to be extracted, socket morphology, periodontal biotype, type of graft material utilized, smoking status of patient as well as oral hygiene compliance.3 When multiple adjacent teeth are being extracted, this can be able to result in increased amount of ridge resorption due to lack of stimulation of the site from loss of multiple adjacent roots of teeth. The use of Xenograft and DFDBA were found to be associated with enhanced ridge augmentation compared to other grafting materials [4]. Additionally, multiple studies have shown that utilizing membrane barriers with bone grafts and bone substitutes significantly improved success of ridge augmentation in both horizontal and vertical dimensions [4,7].
Additionally, in sites with significant bone loss, use of tenting screws has been able to maintain space more effectively allowing for better success with guided bone regeneration by being able to prevent membrane collapse. Tenting screws also protect the augmented site against mechanical injury and favour stabilization of bone and bone substitutes allowing for improved guided bone regeneration [8-10].
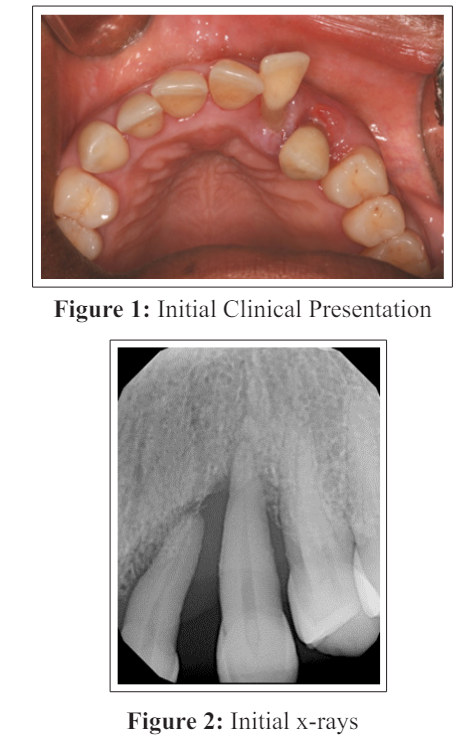
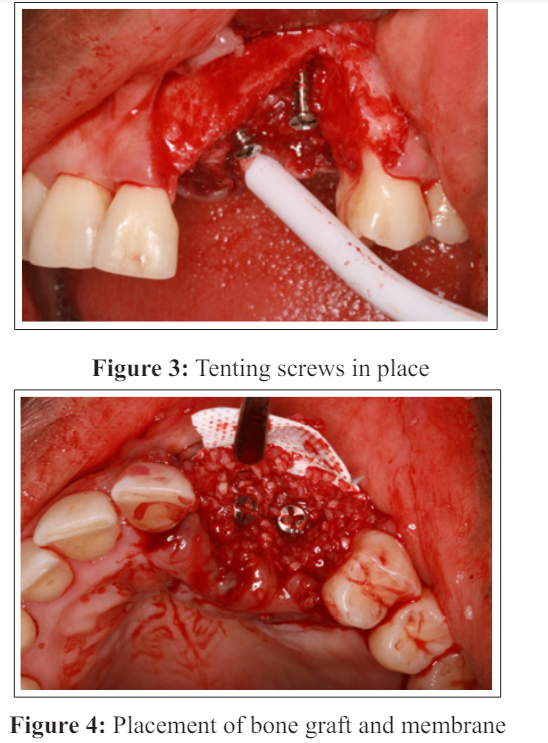
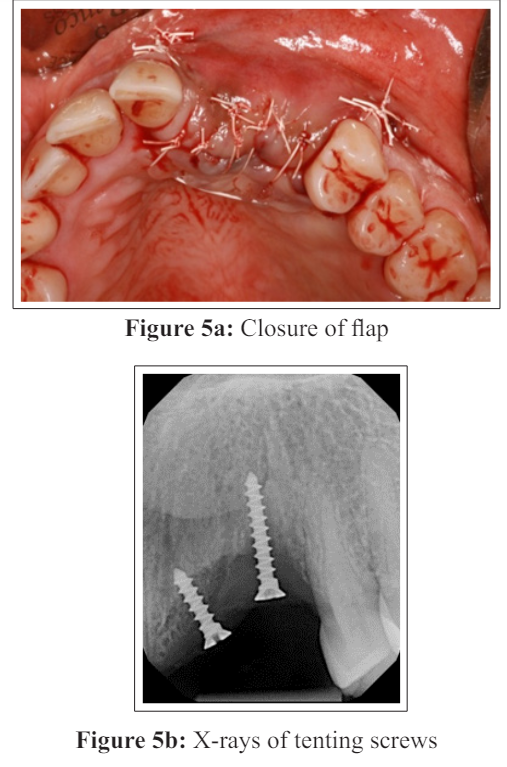
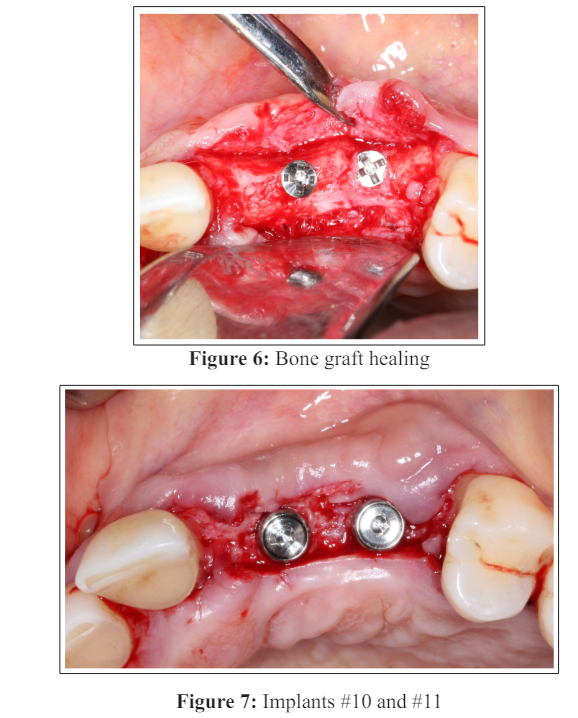
A 45-year-old female was referred to us for emergency treatment. Teeth # 10 and #11 had severe bone loss and mobility and had to be removed. Implant surgery is a very challenging task if teeth are removed due to severe periodontal disease in the esthetic zone because a large visible ridge defect will be created upon removal of the involved teeth causing unesthetic long restorations. (Figures 1 and 2). Teeth # 10 and 11 were removed. (Figure 3) A ridge preservation procedure was then performed to prepare the area for implant surgery utilizing particulate demineralized freeze- dried bone and a titanium reinforced ePTFE membrane. Tenting screws were utilized to correct a severe ridge deficiency by helping creating space for regeneration, allowing increased bone height and width and expanding the soft tissue volume. (Figure 4) This technique enabled guided bone regeneration. (Figure 5a, 5b) An Essix retainer was placed as a temporary restoration. The goal of alveolar ridge preservation is to minimize soft and hard tissue loss following tooth removal and regenerate tissue volume. Following healing, two 3.2X10mm Legacy 2 Implant direct implants were placed.(Figures 6,7 and 8)

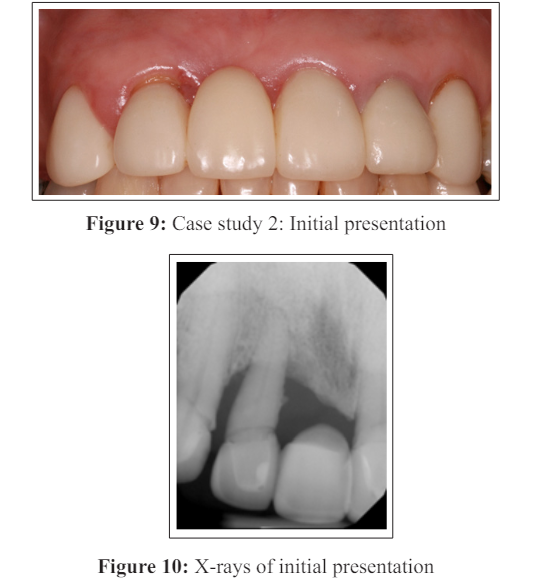
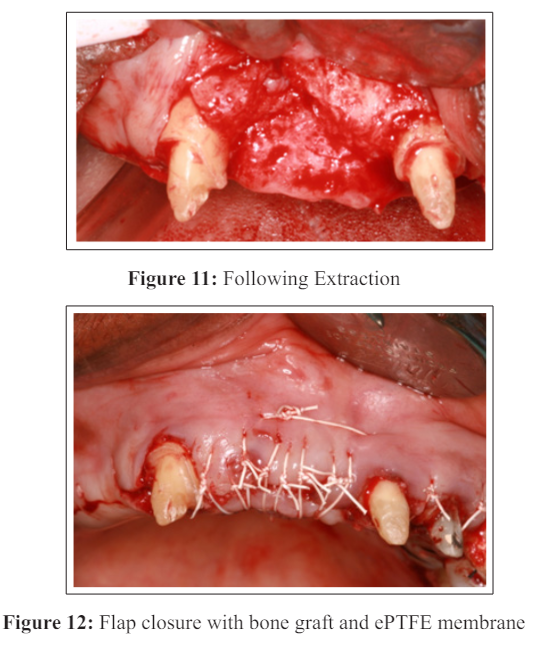
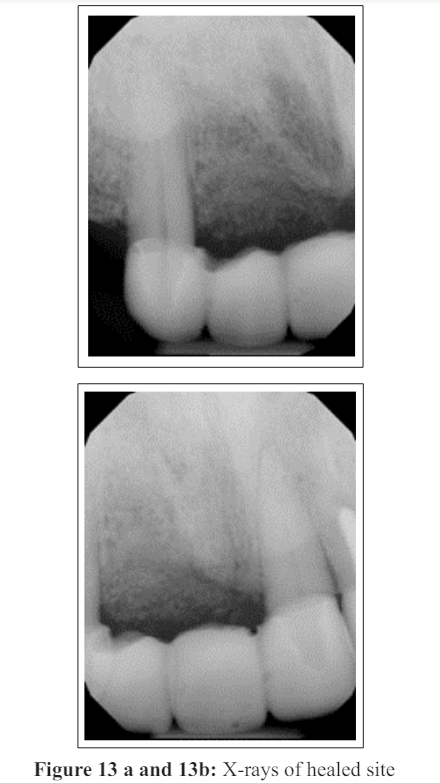
A 77-year-old female presented with pain on maxillary anterior teeth. Clinically, she had a fixed partial bridge from #7-#10. (Figure 9 and 10) Tooth #7 had to be extracted due to periodontal disease and bone loss. Her x-rays showed that the bone loss around tooth #7 would result in significant damage to the socket walls and need for alveolar ridge preservation procedure to prevent bone defects in the esthetic zone. (Figures 11 and 12) To provide a healthy environment for the new fixed restoration, extraction of #7 and alveolar ridge preservation were necessary, as well as crown lengthening for #6 and a new fixed partial ridge from #6- #11. Following extraction of tooth #7, the socket was debrided and demineralized freeze-dried bone and ePTFE membrane was utilized for guided bone regeneration. (Figure 13a and 13b) The goal of the procedure was to maintain ridge contours, and allow placement of an esthetic fixed partial bridge on periodontally healthy teeth. (Figure 14)

Alveolar ridge preservation procedures are utilized to prevent loss of tissue volume in an extraction site following tooth removal. The goal of the procedure is also to use guided bone regeneration principles to regenerate bone for sockets with damaged socket walls allowing maintenance of tissue contours in the extraction site. A number of studies have found a clear benefit to alveolar ridge preservation for retaining dimensions and contours of the extraction sockets compared to extraction sites without ridge preservation especially in sites where esthetics is critical. It also offers the advantage of reducing need for augmentation procedures during dental implant placement. The ability to have space maintenance for barrier membranes and to allow migration of bone cells as well as block other cell types has been important to success of guided bone regeneration. In cases where there is significant loss of bone in the extraction site, use of tenting screws can be helpful in preventing collapse of the membrane allowing maintenance for space with the membrane. Avila-Ortiz and colleagues found that use of Bovine bone and demineralized freeze-dried bone (DFDBA) showed significant advantages in the mid buccal alveolar ridge height compared to alloplastic bone substitutes and also an advantage to use of barrier membrane materials. Being able to have space maintenance to allow adequate guided bone regeneration is essential to success of Alveolar ridge preservation procedures, and use of tenting screws and rigid membranes are important to ensuring adequate space for bone regeneration in damaged extraction site walls.
1. Schropp L, Wenzel A, Kostopoulous L, Karring T (2003) Bone healing and soft tissue contour changes following single tooth extraction: A clinical and radiographic 12 month perspective. Int Journal of Periodontal and Restorative Dent 23: 313-323.
2. Juodzbalyz F, Stumbas A, Gayushar S, Dureal O, Tazum TF 92019) Morphology Classification of Extraction Sockets and Clinical decision tree for socket preservation after tooth extraction. Journal of Oral and Maxillofacial Research 10: E3.
3. Avila-Ortiz G, Chambrone L, Vignoletti F (2019) Effect of Alveolar ridge preservation intervention following tooth extraction: A systematic review and Meta-analysis. Journal of Clinical Periodontology 46: 195-223.
4. Avila-Ortiz G, Elangovan S, Kramer KWO, Blanchette D, Dawson DV (2014) Effect of Alveolar ridge preservation after tooth Extraction: A systematic Review and MetaAnalysis. J of Dental Research 2014;93(10): 950-958.
5. Horowitz R, Holzclaw D, Rosen PS (2012) A review of Alveolar ridge preservation following extractions. Journal of Evidence based Clinical practice 12: 149-160.
6. Macbeth MD, Donos N, Mardas N (2022) Alveolar ridge preservation with guided bone regeneration or socket seal technique. A randomized single blind controlled Clinical trial. Clinical Oral Implant Research 33: 681-699.
7. DeAngelis P, DeRosa G, Manicone PJ, De Giorgi A, Antonio D’Addona, et al. (2022) Hard and soft tissue evaluation of Alveolar ridge preservation compared to spontaneous healing: A retrospective Clinical and volumetric analysis. Int. Journal of Implant Dentistry 8: 62.
8. Neto C, Cavalarti CHF, Sapatta VM, Pannuti CM, Hammerle CHF, et al. (2020) The positive effect of tenting screws for primary horizontal guided bone regeneration: A retrospective study based on Cone beam computed tomography data. Clinical Oral Implant Research 31: 846-855.
9. Daga D, Mehotra D, Mohammad S, Singh G, Nato SM (2015) Tentpole technique for bone regeneration of vertically deficient Alveolar ridges: A Review. Journal of Oral Bio Craniofacial Research 5: 92-97
10. Le B, Rohreh MD, Prassard HS (2010) Screw “Tent-Pole” graft technique for reconstruction of large alveolar ridge defects using human mineralized allograft for Implant site preparation. Journal of Oral Maxillofacial surgery 68: 428- 435.
View PDF