Author(s): Hridya Harimohan* and Mathew Thomas
Snake bites have become a major health concern in India. The American Society of Tropical Medicine and Hygiene said in India 46,000 people are dying every year from snake bites against the official figure of only 2000 [1]. Aplastic anemia is a rare hematological disorder where bone marrow fails to produce blood cells due to decrease in the bone marrow stem cells. In about more than 60% of cases the cause of bone marrow failure is not known and is called idiopathic aplastic anemia. Several cases are due to various secondary causes including inherited aplastic anemia, radiotherapy, chemotherapy, viral infections (EBV,CMV,HIV) and chemicals like benzene. We are reporting a case of a young boy with no comorbidities who had a poisonous snake bite with serious envenomation and developed severe aplastic anemia during the course of the hospital stay. Aplastic anemia recovered during follow up. To our best knowledge and search, we could not find a similar case in literature.
17-year-old previously healthy boy with no comorbidities presented to the emergency department with a history of suspected snake bite on his right big toe on 25th March 2018. On examination, he was fully conscious and was able to convey the history. His vitals signs were an arterial pulse of 142/min, blood pressure of 140/80mm of Hg, respiratory rate of 30/min, temperature of 102 F. Physical examination showed a hematoma of size 2*2 cm on right big toe, bilateral subconjunctival hemorrhage and edema. There were several other areas of ecchymosis found over his body. Respiratory examination on auscultation showed decreased breath sounds on both sides suggestive of bronchial spasm. Examination of neurological and other systems were normal. While still in the emergency department, he desaturated suddenly with oxygen saturation of 74% in ambient air. He was immediately intubated in the emergency department in view of impending respiratory arrest. He was later shifted to the medical intensive care for close monitoring and treatment.
Investigations showed features of severe DIC (abnormal PT, aPTT, decreased platelets and decreased fibrinogen, increased FDP, D dimer) for which he was given several units of blood products (FFP, PRBC and platelets). He was also given appropriate doses of anti snake venom. In intensive care he developed severe sepsis and multiorgan dysfunction. Culture showed Acinetobacter baumannii and was on Meropenem and Teicoplanin. He also underwent renal replacement treatment for acute kidney injury (AKI). Blood investigations showed altered RFT: creatinine 6.7, INR 13, aPTT 48 seconds, elevated BT 8.9min and CT 16.5min. ABG showed metabolic acidosis with Ph 7.1, bicarbonate 12 and pCO2 30 and lactate 42. Potassium 3.3, Sodium 133. Altered LFT with AST 59 ALT 93. Toxicology screen and infectious screening, ANA profile was negative, Procalcitonin was 36.1 ng/ml. (Normal<0.1ng/ ml). Chest Xray showed bilateral opacities suggestive of Acute Respiratory Distress Syndrome. ECHO showed impaired diastolic dysfunction. During the course of the treatment, his sepsis cleared but we noted that he developed severe pancytopenia in spite of several units of blood products like PRBC and platelets and even after the stoppage of suspecting antibiotics.
| Day in thehospital | Hemoglobin (g/dl) | WBC (cubic mm) [ANC] | Platelet Count |
| Day 1 | 6.4 | 8800[6400] | 23,000 |
| Day 2 | 6.9 | 10,300[7600] | 21,000 |
| Day 9 | 5.5 | 3600[1900] | 12,000 |
| Day 10 | 6.9 | 4700[2100] | 12,000 |
| Day 11 | 7.7 | 3400[1700] | 14,000 |
| Day 12 | 7.2 | 2900[1700] | 8000 |
We did a bone marrow aspiration and trephine biopsy. Bone marrow aspiration showed dilute marrow with occasional scattered normoblast, scattered myeloid cells and absent megakaryocytes The trephine biopsy showed severe aplastic anemia with the marrow cellularity around 10% which was quite surprising (Figure 1). At this point, a discussion with relatives were done and options for treatment including bone marrow transplantation were conveyed to them. Meanwhile the patient became better with supportive treatment. He became clinically better, especially the bleeding tendencies. His coagulation parameters started returning to normal. He was extubated on the 10th day of his hospital course. His urine output increased and dialysis was weaned off. The blood counts increased and his discharge was planned. At the time of discharge, his blood counts Hb 11.7g/dl, WBC 4100 per cubic mm, ANC 2460 and platelet 3,41,000.
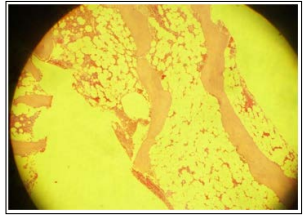
Figure 1
He was discharged and asked to come for regular follow up. After one month, the bone marrow was repeated which showed a remarkable recovery with 50-60% cellularity and normal trilineage hematopoesis. (Figure 2). He is still on follow up. The last follow up was on 01 February, 2019 and the blood counts were Hb 12.1g/ dl, WBC 5800 per cubic mm, ANC 2000 and platelet 2,16,000. Other blood parameters were normal
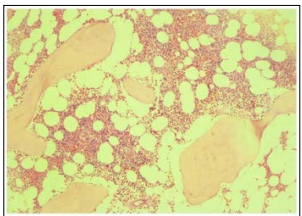
Figure 2
Although the snake was not identified in this case, this patient was most likely envenomated by viper because of serious bleeding manifestation and renal involvement requiring dialysis. The wellknown complications of viper bite are DIC, Acute Tubular Necrosis, sepsis due to infection at the bite site leading to the Multi Organ Dysfunction. This patient has a very rare manifestation of snake bite producing severe aplastic anemia. To our best knowledge we could not find a similar case reported in literature. Any mechanisms postulated for aplastic anemia are futile because of the lack of cases in the literature. Variations in the constituents of snake venom have been reported by many according to the geographical distribution in India. For example, some of the viper bites may cause some neurological symptoms and some of the krait and cobra bites may cause some hematological symptoms. This patient was lucky to have a reversible Bone Marrow aplasia which is not common in the short period of time without specific treatment whatever be the cause. It may be better to keep the patient on a long term follow up as many other similar circumstances (like drugs, chemicals, infections etc) could lead to a suppression of Bone Marrow in this patient again.
Phenomenon of interspecies variations in the snake venom has been well documented in India [2]. It is possible that the variation in the constituents in the venom may account for the pathology in our case. Any unusual constituent which could have suppressed the bone marrow temporally either directly or through immunological mechanisms could be postulated as the cause in our case. What that particular unusual constituent was, remains a mystery