Author(s): Shambavi Bojja, Vennela Borra, Alka Bhingardeo*, Mrudula Chandrupatla, Ayush Amlan and Abdul Wahid Ansari
Variations in the intrinsic muscles of sole are relatively uncommon. There are 18 intrinsic and 4 extrinsic tendons in the sole of foot. These muscles are subjected to variations which are usually encountered during surgery or cadaveric dissections. During routine cadaveric dissection we came across a combination of variations in sole dissection. There was variation in number of flexor digitorum brevis and variation in the origin of flexor digitorum accessorius. The intertendinous connection between flexor digitorum longus and flexor hallucis longus was also observed. The flexor digitorum brevis muscle, in particular its fourth slip, has a significant clinical and surgical importance in medical practice. The knowledge of the frequency of flexor digitorum brevis fourth slip agenesis and variations in relation to the demographic characteristics of patients is of importance for tendon repair, tendon transfer or soft tissue reconstruction in foot surgery. The exact anatomical knowledge of crossing of Flexor Digitorum Longus and Flexor Hallucis Longus in the foot is essential to facilitate tendon harvesting with less morbidity and explain possible reasons for postoperative functional loss. The understanding of variations of sole muscle is very useful to orthopedic surgeons, radiologists and podiatrists for analyzing foot function and for biomechanical modeling of the foot.
Human sole anatomy is highly intricate and comprises of various muscles, nerves and vessels arranged into 4 layers. Abductor hallucis, flexor digitorum brevis, abductor digiti minimi are usually reflected in the first layer [1]. The flexor digitorum brevis generally originates from calcaneum, divides into four tendons and gets inserted on lateral four toes. It is found to have many variations in course of its termination. In our case, we found a bilateral variation of absence of fourth tendon of flexor digitorum brevis. According to the case reported by Isurani Ilayperuma absence of FDB tendon to 5th toe was observed in 72% of the study subjects. According to a case study by Andrew Bernhard on a pool of 60 cadavers, 48% of them lacked FDB tendon to 5th toe. The knowledge of variations of flexor digitorum brevis would be of immense clinical significance for tendon repair via tendon transfer to correct deformities such as claw toe or hammer toe or soft tissue reconstruction in foot surgery [2-5].
Flexor digitorum longus, flexor digitorum accessorius, lumbricals and flexor hallucis longus form the second layer in the sole. The flexor digitorum accessorius or quadratus plantae arises from calcaneum and gets inserted on the tendon of flexor digitorum longus [1]. The knowledge of high variability of this muscle holds a significant importance to surgeons who perform foot reconstructive surgery [6]. We observed a case of non-union of both heads of quadratus plantae before it’s insertion onto flexor digitorum longus.
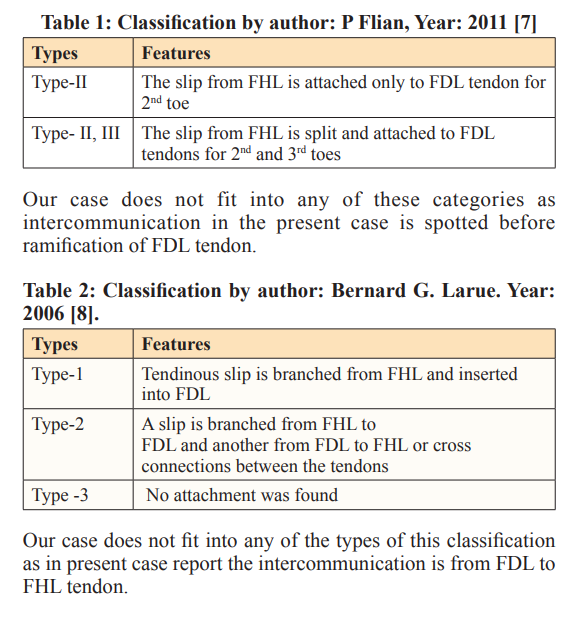
The flexor digitorum longus (FDL) arises from tibia and inserts on to the distal phalanges of lateral four toes by dividing into four tendons while the flexor hallucis longus (FHL) arises from fibula and get inserted onto the distal phalanx of great toe [1]. We observed cross connection between the tendons of flexor digitorum longus and flexor hallucis longus in both feet. The intertendinous connections between flexor digitorum longus and flexor hallucis longus is one of the common variations observed in the foot. The author, P Filan had reported such intertendinous connection between FHL and FDL in his study [7]. Precise knowledge of the anatomy of the crossing of FDL and FHL in the plantar foot is essential to facilitate tendon harvesting, reduce morbidity and explain possible postoperative functional loss [8]. Present case report is a unique combination of variations of flexor digitorum brevis, flexor digitorum accessorius, intertendinous connections between flexor digitorum longus and flexor hallucis longus. Knowledge of such variations is important to radiologists, orthopedicians and surgeons.
During routine cadaveric dissection of sole of a 50-year-old female cadaver after removing skin and fat and reflecting plantar aponeurosis, in first layer we surprisingly found a bilateral variation of 3 tendons of flexor digitorum brevis instead of four tendons. The fourth tendon of flexor digitorum brevis going to 5th toe is missing. The three tendons are inserted onto the sides of middle phalanges of second, third and fourth toes. There is no variation in nerve supply and is supplied by medial plantar nerve (S1, S2).
As we continued with the dissection in the second layer we noticed non-union of medial and lateral head of flexor digitorum accessorius during its insertion onto flexor digitorum longus in right sole of the cadaver. We observed that medial and lateral heads are inserted separately onto flexor digitorum longus. Medial head is smaller and inserted on the superficial surface (close to 1st layer) of tendon of flexor digitorum longus and lateral head is larger and inserted on deeper surface of tendon (close to third layer). Insertion of both heads are proximal to branching and on lateral side of tendon of flexor digitorum longus. No such variation is observed in other sole (unilateral variation). The nerve supply was normal and was by lateral plantar nerve (S2, S3).
As we proceeded with the dissection of third layer we found intertendinous connections between flexor digitorum longus tendon and flexor hallucis longus tendon at Henry’s knot (where flexor digitorum longus crosses the flexor hallucis longus) in both the soles. There is a single tendinous slip connecting both tendons going proximally to distally from flexor digitorum longus to flexor hallucis longus. Both the muscles are supplied by tibial nerve (L4, L5, S1, S2, S3) as described in the general literature.
Numerous anatomical variations of flexor digitorum brevis that differed from classical descriptions in anatomy texts are not uncommon. In our case absence of tendon of FDB to fifth toes without any supernumery slips was observed. Similar variations were reported by Kaissar yammine, Jailenne I. Quinones- Rodriguez, S W Lobo, Isurani Ilayperuma. On the contrary, Rajesh tangarajan in his article had mentioned that the fourth tendon of FDB is replaced by isolated flexor muscle originating from main muscle belly before it’s division into tendons. While reviewing other articles, it was found that the tendon of FDB to fifth toe is replaced by musculotendinous slip arising from FDL. Also, sometimes a slip from very thin separated muscle belly originating from intermuscular septum as flat fascia under FDB replacing the absent tendon of FDB have been reported. The absence of fourth tendon of FDB does not affect locomotor functions in human much, as compared to chimpanzees or other hominoids. When compared to the little finger, the little toe has less function and opposition is absent in humans. Hence, we can say that the muscles acting on the little toe are undergoing evolutionary changes. The action of FDB can be compensated by other long flexors of the foot. This could have resulted due to gradual reduction in the usage of the little toe as the bipedal posture evolved in. Paralysis of flexor digitorum brevis may result in distortion of arches of foot. Claw toe instability at the proximal interphalangeal joint may be corrected by an FDB tenotomy. Sound knowledge about variations in flexor digitorum brevis is useful in tendon transfer surgeries of claw toe and hammer toe. The knowledge of variations of FDB is also used in soft tissue reconstruction in foot surgery and diagnostic imaging for soft tissue of foot to minimize the error during treatment. This information is also significant in transfer of musculocutaneous flap for heel pad reconstruction. In procedures like the Valtin approach, the FDB is used to replace FDL tendon that has been shortened and lost its function due to ischemic muscle contracture. With this technique, it is possible to restore flexion in the patients. Also, the FDB muscle is used as one of the three intrinsic foot muscles to cover diabetic foot wounds through local flaps for foot reconstruction. This surgical intervention can be used for coverage of minor foot defects such as calcaneal defects. Curly toe is a common congenital deformity characterized by flexion and varus deformity of the inter-phalangeal joints. Flexor digitorum brevis tendon has also been used successfully in the surgical correction of this condition [2-6, 9-12].
Flexor digitorum accessorius (FDA) is the muscle of the second layer of the sole [1]. Non-union of medial and lateral heads of FDA is observed in our case. To the best of our knowledge, no similar variation was found in literature search. Other variations of insertion of FDA to one of the slips of FDL or FHL had been reported. Understanding the high variability of FDA muscle is of great importance to surgeons who perform foot reconstructive surgery. Sometimes there may be presence of an accessory muscle known as flexor digitorum accessorius longus (FDAL). There are many variant types of this accessory muscle. Different classifications systems on the variations of FDAL were also proposed. The FDAL is intimately related to the neurovascular bundle and may abut, compress, or impinge upon the posterior tibial and/or lateral plantar nerves. Accessory muscles of the ankle are typically asymptomatic, but can cause pain, compressive neuropathy, compartment syndrome, or rigid hind foot deformities, and can also mimic soft tissue tumors [13-18].

Figure 1: Presence of only three tendons of Flexor Digitorum Brevis
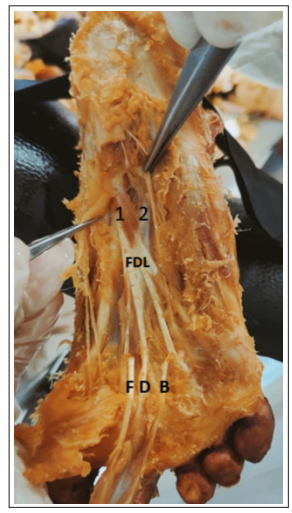
Figure 2: Non-union of two Heads of FDA
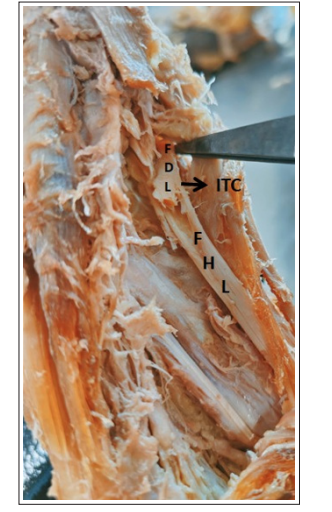
Figure 3: Intertendinous Connection between FDL and FHL
The flexor hallucis longus (FHL) and flexor digitorum longus (FDL) tendon are routinely used in reconstructive foot and ankle surgery [20]. These tendons show variable intertendinous connections while crossing in the chiasma plantare.
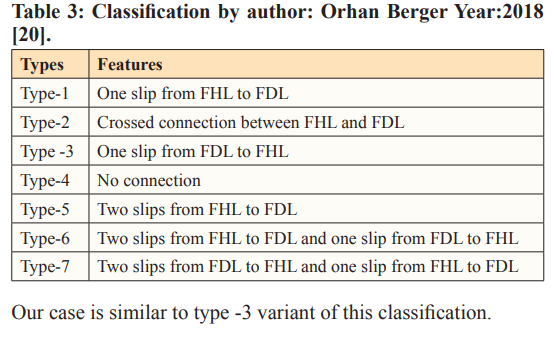
Various classifications of intertendinous connections between flexor digitorum longus and flexor hallucis longus have been proposed.
Various classifications of intertendinous connections between FDL and FHL:
In some cases, there was an observation that the tendinous slip given by FHL to FDL may be proximal or distal to master’s knot of Henry. When tried to correlate embryologically, author Masahito YAMAMOTO mentioned in his article that FHL and FDL arise from the at deep side of navicular bone. Therefore, in the common plate in human embryos and fetuses, much or less, some connections between tendons seemed to remain even after birth. Tendon transfer of the FHL and the FDL is an established procedure for the treatment of achilles tendinopathy or tendon rupture. Sometimes this transfer is also used in the treatment of tibialis posterior muscle dysfunction, posterior foot balancing in neuromuscular foot deformities. These interconnections between FHL and FDL have great significance in ankle and foot reconstruction surgeries like chronic Achilles tendon rupture, posterior tibial tendon Dysfunction (PTTD) and peroneal tendon rupture. As described by Srinivas Rao et al among both the flexor tendons FHL tendon is frequently used in the treatment of chronic Achilles tendinopathy, whereas Posterior tibial tendon deficiency (PTTD) is frequently treated with FDL tendon graft transfer along with associated bony procedures. The variable intertendinous connections between the flexor tendons while crossing the chiasma plantarae can complicate harvesting of tendons. Surgical debridement of the Achilles tendon with transfer of FHL tendon has shown significant improvement in Achilles tendon functioning and reduction of pain in the patients and even Post-operative functional loss of FHL tendon even after the transfer is minimal. The exact anatomical knowledge of crossing of FDL and FHL in the foot is essential to facilitate tendon harvesting with less morbidity and explain possible reasons for postoperative functional loss. The restoration of function of a deficient tibialis posterior tendon in stage II adult acquired flat foot deformity (AAFD) is often attained by tendon transfers of FHL and FDL [7, 8, 21-29].
Variations in sole are not uncommon. The FDB muscle is used as one of the intrinsic foot muscles to cover diabetic foot wounds through local flaps for foot reconstruction. The knowledge of variations in flexor digitorum brevis is useful in tendon transfer surgeries of claw toe and hammer toe. Information of crossing of FDL and FHL in the foot is essential to facilitate tendon harvesting with less morbidity. The anatomical knowledge of variations of sole muscle is very important to orthopedic surgeons, radiologists and podiatrists for analyzing foot function, biomechanical modeling of the foot and prosthesis designing.
Present case report is about findings in our routine dissection of lower limb in cadaver during First MBBS teaching session. This is exempted from Ethics approval.
We don’t have any Competing interests.
Author Shambhavi and Vennela - Contributed in writing case report and discussion Author Dr. Alka - Identified Variation, Abstract, Diagram, Conclusion and guided author Shambhavi and Vennela in writing case report and discussion Author Dr. Mrudula - Contributed in Introduction Author Ayush and Wahid contributed in Introduction All authors reviewed the manuscript
No funding involved.
Not applicable
1.Standring S, Standring Susan (2020) Gray’s Anatomy, the Anatomical Basis of Clinical Practice, 42nd Ed. Spain: Churchill Livingstone Elsevier 1421-1457.
2.Ilayperuma I (2012) On the variations of the muscle flexor digitorum brevis: anatomical insight. Int. J. Morphol 30: 337-340.
3.Andrew Bernhard, Josh Miller, Jason Keeler, Kathy Siesel, Evan Bridges, et al (2013) Absence of the fourth tendon of the flexor digitorum brevis muscle: a cadaveric study. Foot Ankle Spec 6: 286-289.
4.Jailenne I, Quiñones-Rodriguez, Cristian Mantilla-Rosa, Félix Rodríguez, Catalina I. Villamil, Juan Fernández, et al (2022) A Missing Flexor Digitorum Brevis Tendon and It’s Relationship to Sex and Ancestry: Evolution in Hespanic Population. Anatomia 1: 210-216.
5.Ramesh Rao, Suresh R Rao (2017) Variation in the Origin of Flexor Digitorum Brevis – A Case Report. Journal of Applied Life Sciences International 11: 1-4.
6.Shweta Talhar, Bharat Ramrao Sontakke, Vandana Wankhede (2017) A rare variation of flexor digitorum accessorius insole and its phylogenetic significance. January 2017 • Journal of Mahatma Gandhi Institute of Medical Sciences 22: 44.
7.P Filan, R Hart (2011) Relationship of the flexor hallucis longus and flexor digitorum longus tendons in the plantar midfoot. An Anatomical cadaver study. Acta Chir Orthop Traumatol Cech 78: 71-76.
8.LaRue BG, Anctil ÉP (2006) Distal Anatomical Relationship of the Flexor Hallucis Longus and Flexor Digitorum Longus Tendons. Foot & Ankle International 27: 528532.
9.Kaissar Yammine (2015) The fourth slip of the flexor digitorum brevis muscle of the human foot. A systematic review and meta-analysis. Ital J Anat Embryol 120: 59-70.
10.Lobo SW, Menezes RG, Mamata S, Baral P, Hunnargi SA, et al. (2008) Phylogenetic variation in flexor digitorum brevis: a Nepalese cadaveric study. Nepal Med Coll J. 10: 230-232.
11.Rajesh Thangarajan, Pugazhandhi Bakthavatchalam, Bhagath Kumar Potu, Huban Thomas (2010) Anatomical variation of the flexor digitorum brevis muscle revisited: a case report from South Indian population. International Journal of Anatomical Variations 3: 211-213.
12.Bülent Yalçin, Hasan Ozan (2005) Some variations of the musculus Flexor digitorum brevis. Anatomical Science International 80: 189-192.
13.Lokesh A Coomar, Daniel T Daly, Jay Bauman (2022) A Unique Variation of Quadratus Plantae in Relation to the Tendons of the Midfoot. J. Funct. Morphol. Kinesiol 7: 49.
14.Jorge Pablo Batista, Jorge Javier del Vecchio, Pau Golanó, Jordi Vega (2015) Flexor Digitorum Accessorius Longus: Importance of Posterior Ankle Endoscopy. Case Reports in Orthopedics 2015: 4.
15.John F Carroll (2009) Accessory Muscles of the Ankle. MRI Web Clinic: https://radsource.us/accessory-muscles-of-the-ankle/.
16.Matthew Holzmann, Noor Almudallal, Kelsey Rohlck, Rohit Singh, Sungho Lee, et al (2009) Identification of a flexor digitorum accessorius longus muscle with unique distal attachments. Foot 19: 224-226.
17.Sobana Mariyapan, Geeta Anasuya D, Sheela Grace Jeevamani, Vijaianand M (2021) An Erratic Origin of Quadratus Plantae: An Embryological ErrorAn Erratic Origin of Quadratus Plantae: An Embryological Error. Int J Anat Res 9: 8168-8172.
18.DustinC Lin, Raissa Zuim Dantas De Souza, Ann Fefferman, Vincent Baribeau, et al (2021) Unusual bilateral variation of the flexor digitorum accessorius longus muscle and its relation on tarsal tunnel syndrome. Surg Radiol Anat 43: 2083-2086.
19.Mi-Sun Hur, Hyung-Sun Won, Chang-Seok Oh (2014) Classification system for flexor digitorum accessorius longus muscle variants within the leg:clinical correlations. Clin Anat 27: 1111-1116.
20.Orhan Beger, Özlem Elvan, Mert Keskinbora, Burçin Ün, Deniz Uzmansel, et al (2018) Anatomy of Master Knot of Henry: A morphometric study on cadavers.Acta Orthopaedica et Traumatologica Turcica 52: 134-142.
21.Perin Wan-ae-loh, Pimpimol Dangintawat, Thanasil Huanmanop, Sithiporn Agthong, Vilai Chentanez (2020) Anatomical Variation of Tendinous Interconnection between Flexor Hallucis Longus and Flexor Digitorum Longus Tendon and Its Location Regarding Master Knot of Henry. The FASEB Journal 34: 1-1.
22.Srinivasa Rao Sirasanagandla, Varna Taranikanti, Raghu Jetti (2018) A Complex Cross Link between the tendons of Flexor Hallucis Longus and Flexor Digitorum Longus. Journal of Morphological Sciences 35: 177-179.
23.Yamamoto M, Shiraishi Y, Kitamura K, Zhe Wu Jin, Gen Murakami, et al. (2016) Early embryonic development of long tendons in the human foot. Okajimas Folia Anat Jpn 93: 59-65.
24.Bergman RA, Thompson SA, Afifi AK, Saadeh FA (1988) Compendium of Human Anatomic Variation. Urban & Schwarzenberg, Munich 300-318.
25.Mao H, Dong W, Shi Z, Weigang Yin, Dachuan Xu, et al. (2017) Anatomical Study of the Neurovascular in Flexor Hallucis Longus Tendon Transfers. Sci Rep 7: 14202.
26.Manikanta Reddy, Vallishri V, Lakshmi Devi CH (2019) Study on tendinous connections between flexor hallucis longus and flexor digitorum longus. Int J Anat Res 7: 6531-6535.
27.Plaass C, Abuharbid G, Waizy H, Ochs M, Stukenborg- Colsman C, et al. (2013) Anatomical variations of the flexor hallucis longus and flexor digitorum longus in the chiasma plantare. Foot Ankle Int 34: 1580-1587.
28.Schon LC, Shores JL, Faro FD, Vora AM, Camire LM, et al. (2013) Flexor hallucis longus tendon transfer in treatment of Achilles tendinosis. J Bone Joint Surg Am 95: 54-60.
29.Backus JD, McCormick JJ (2014) Tendon transfers in the treatment of the adult flatfoot. Foot Ankle Clin 19: 29-48.
View PDF