Author(s): Lina Ramírez Páez* and Norma E. Ávila Portillo
Taurine, a semi-essential amino sulfonic acid, is present in high amounts in the retina. It has anti-inflammatory, antioxidant, and neuromodulatory properties which have shown to be beneficial for specific neurodegenerative conditions [1]. However, its effects on high myopia or its complications are unknown. We report the case of a 60-year-old woman with pathological myopia, who 7 years ago, presented a best corrected visual acuity (BCVA) of 20/200 right eye (OD) and 20/70 left eye (OS), and was diagnosed with a choroidal neovascular membrane (CNV) OS. She initiated taurine supplementation (1.5 g/daily for 14 days) and improved to a BCVA of 20/100 OD. She continued taking 500 mg/daily. Subsequent events included 4 injections of Aflibercept OS, cataract surgery in both eyes (AO), and peripheral retinal photocoagulation in AO. This last treatment induced a severe inflammation and loss of visual acuity OS. She was treated with corticosteroids, but after two weeks due to lack of improvement, the taurine dose was increased to 1 g/day. Three weeks after, her BCVA went from counting fingers to 20/60 OS, and her inflammation was controlled. After 7 years of continuous taurine intake, her CNV OS has remained inactive, her BCVA was stable and even improved in the last year from 20/45 OD and 20/80 OS to 20/25 OD and 20/60 OS, respectively. At the same time, her migraines decreased in intensity and frequency. This case report brings a new light towards the potential use of taurine supplementation in high myopia, retinal degeneration, and pathologic myopia.
Myopia (aka, nearsightedness) is a refractive error, signaled with a negative spherical equivalent correction (e.g. -0.50 D) when ocular accommodation is relaxed. High myopia refers to a spherical equivalent refractive error of ≤ - 6.00 D and pathologic myopia refers to a structural changes in the eye, secondary to myopia, that may lead to loss of vision, Figure 1 [2]. In 2020 it is estimated that 2.5 billion people worldwide will have myopia [3]. Treatment of myopia includes optic (spectacles, contact lenses, or refractive surgery), pharmacological (Atropine, Pirenzepine, etc.), and surgical corrections, none of which is a definitive treatment to improve vision or to avoid myopia progression [4].
Taurine is a semi-essential, sulfonic amino acid, found in meat (specially uncooked) [5]. Self-body production is insufficient, and often reduced with aging. Among its different biological functions are the improvement of the immune system, the endocrine system, and the central nervous system, where it works as a neuroprotective agent. Taurine promotes the development of fetal brain tissues and the proliferation, differentiation, maturation, and survival of neural stem cells (NSCs) [6, 7]. Therefore, it has been studied in diseases like epilepsy, glaucoma and optic neuropathy with encouraging results. In the retina, taurine’s deficit is related to gyrate atrophy, and it has been suggested as a supplement in the treatment for retinitis pigmentosa [8, 9, 10, 1].
Environmental and genetic causes are linked to myopia. At a molecular level, oxidative stress and hypoxia are well known pathophysiologic mechanisms that underlie high myopia development [4] and finally lead to retinal degeneration Figure: 1 [11]. These mechanisms promote molecular changes in the sclera, choroids, and retina that cause retinal remodeling and development of the eye’s axial elongation [11]. Complications of high myopia are glaucoma, posterior staphyloma, photoreceptor degeneration, optic neuropathy, and myopic maculopathy (e.g. choroidal neovascular membrane). All these complications lead to visual loss [4].
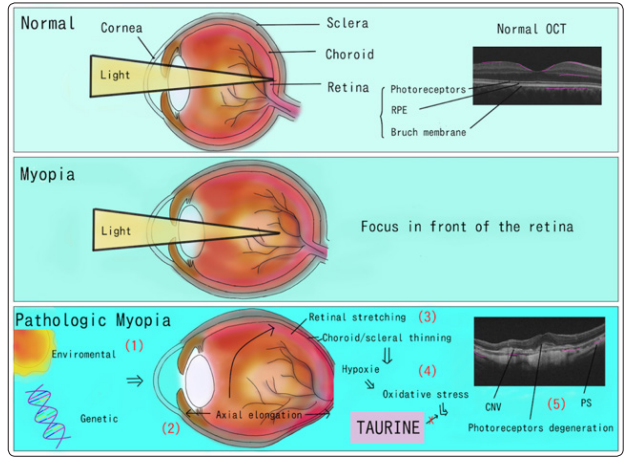
Figure 1: Comparison between a normal and a myopic eye. Pathophysiology of pathologic myopia (events enumerated). Normal OCT (optical coherence tomography) shows a flat retina. CNV: choroidal neovascular membrane. PS: posterior staphyloma (posterior bulging of the globe). Lina Ramírez
In animal studies, taurine exerts an antioxidant effect in (CNV) OS. Her visual acuity drastically decreased to 20/200 OD, 20/70 OS. The patient decided to start taurine supplementation at 1500 mg/daily divided into two doses for 14 days, after that the BCVA improved to 20/100 OD and the OS remained without changes.
Subsequent events included: treatments with 4 intravitreal injections of Aflibercept (Eylea) OS, an Anti-VEGF, (in space of 8 months after diagnosis) and cataract surgery in AO. She kept on taking taurine at 500 mg/daily fasting. She remained asymptomatic and as an additional finding, reported improvements in the frequency and severity of her migraines compared to prior initiation of taurine.
At age 59, she underwent peripheral retinal photocoagulation in both eyes and her visual acuity severely decreased to counting fingers OS. The patient was treated with one dose intramuscular corticosteroid injection and prednisolone eye drops, but after 2 weeks her visual acuity improved slightly. Therefore, the patient increased to 1 g/day of taurine, 3 weeks after, inflammation was controlled (under the slit lamp) and her BCVA changed from counting fingers to 20/60 OS. photoreceptors, ganglion cells, and Muller cells an anti- inflammatory effect and a cytoprotective effect on retinal ganglion cells since it regulates cellular calcium influx [9, 6, 12, 1].
High myopia is increasing worldwide, and the quality of life in these patients is often reduced [3,4]. A definitive treatment for high myopia or to prevent myopia progression is not yet established, and although taurine works in many diseases, its effect in high myopia and/or its complications needs to be evaluated. In the present report, we describe a case of pathologic myopia AO in an adult patient who strictly complied with taurine supplementation for 7 years, to control her high myopia and its complications.
The patient is a 60-year-old woman, veterinarian, MSc. Animal nutrition, who at age 16 was diagnosed with high myopia with -14 D both eyes (AO). Relevant medical history is positive for migraine without aura for 20 years, and osteopenia for the last 2 years. Her ophthalmological history is positive for photocoagulation of peripheral retinal holes and LASIK (refractive surgery) AO.
At age 53, she attended her retina specialist for evaluation of metamorphopsia (distorted vision) in her left eye (OS), who after comprehensive ophthalmological examination, including fluorescein angiography and optical coherence tomography (OCT), diagnosed cataract OD and choroidal neovascular membrane After 7 years of continuous intake of taurine: the choroidal neovascular membrane (CNV) OS has remained inactive (Figure 2), and her visual acuity remained stable and even improved with 1 g/daily, it changed from 20/45 OD and 20/80 OS to 20/25 OD and 20/60 OS (Table 1).
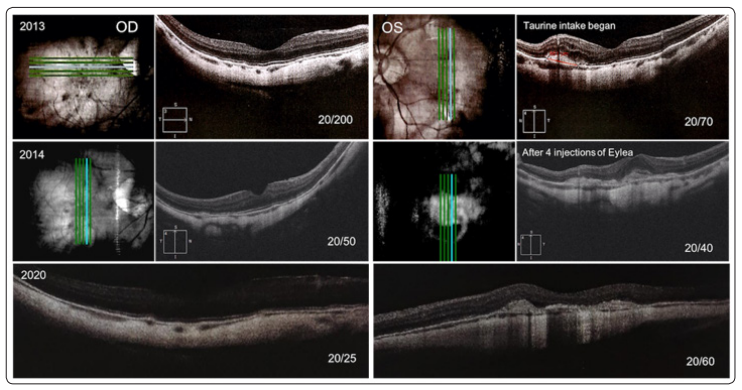
Figure 2: Follow up with Optical Coherence Tomography
AO posterior staphyloma. OD light epiretinal membrane. OS inactivity of choroidal neovascular membrane during observation. Visual acuity not to be expected from anatomy OS. Last images not at the fovea (images obtained from health insurance company)
|
Date |
OD |
Subjective refraction |
OS |
Subjective refraction |
|
April 10th 2013 |
20/200 |
* |
20/70 |
* |
|
April 27th, 2013 |
20/100 |
- 3.0 - 1.0 x 75° |
20/70 |
- 1.0 - 1.5 x 175° |
|
August 29th, 2013 |
20/30 |
* |
20/30 |
* |
|
March 10th, 2014 |
20/50 |
- 2.75 - 1.50 x 75° |
20/40 |
- 1.0 - 1.50 x 180° |
|
July 10th, 2019 |
20/45 |
* |
20/80 |
* |
|
April 9th, 2020 |
* |
* |
CF |
* |
|
April 30th, 2020 |
20/30 |
* |
20/60 |
* |
|
May 8th , 2020 |
20/25 |
+ 3.75 - 2.0 x 80° |
20/60 |
+ 2.50 - 0.75 x 150° |
OD: right eye. OS: left eye. CF: counting fingers * Data not available
Although the patient tried to stop the use of taurine several times during this 7-year time period, she realized that after a while, her visual acuity was reduced. Therefore, she continued with taurine supplementation until present.
Additional relevant history throughout this time includes a strict diet with the goal to reduce migraine episodes as well as improve her vision, which was the introduced prior to taurine initiation. She avoided the consumption of chocolate, coffee, and fruits (i.e., banana and papaya) that were known triggers for her migraine. She also avoided eating saturated fat. Additional supplements in her diet included 400 mg vitamin E, non-specific vitamins and minerals, and calcium 600 mg daily.
Taurine is a semi-essential amino acid that may play an important role as a neuroprotector in neurodegenerative processes. The present case suggests its potential benefit on high myopia when provided as a supplement, and pathologic myopia’s control as evidenced by visual acuity improvement and subsequent stabilization, as well as OCT stable findings for CNV disease.
Previous studies demonstrate that prognosis in high myopic patients is poor, those are evidenced by visual acuities of 20/200 or even worse in patients with CNV, where 96% of patients have a poorer prognosis within 5-10 years [13, 4, 3]. According to Ripps and Shen taurine is the most abundant amino acid in the ciliary body, iris, cornea, lens, retina, and vitreous [8]. It is essential in the development of photoreceptors and acts as a cytoprotectant against stress-related neuronal damage. Since oxidative stress and hypoxia are well known pathophysiologic mechanisms that underlie high myopia development and finally lead to retinal degeneration, taurine may have worked as a cytoprotectant against stress- related neuronal damage and may have maintained a good visual acuity in this case.
Table 1 shows two times period when taurine could have improved her visual acuity: 1. OD improved between the first and second measurements, when the only treatment was 1.5 g taurine/daily for 10 days; and kept on taking 500 mg/daily, it showed stabilization for 7 years. 2. both eyes improved between the fifth and sixth measurements, when she increased the dose from 500 mg to 1 g/daily. Taurine may have worked as a cytoprotectant against stress- related neuronal damage and may have maintained a good visual acuity.
Myopia progression can be measured through the ocular axial length and/or the refractive defect. How could taurine avoid myopia progression? It may be argued through 3 mechanisms, first, as an antagonist of GABAc receptors; second, as a dopamine synergist, and third, as an antioxidant.
First, retinoic acid is a known ocular growth regulator [14]. GABAc receptor antagonists i.e, cis- and trans-3-ACPMPA, (cis- and trans-3-aminocyclopenta- nyl methylphosphinic acid) prevented myopia development in experimental studies with chicken, possibly through the interaction with the retinoic acid pathway in the retina [15]. A study with a guanidine analog of taurine, the 2-guani- dinoethanesulfinic acid (taurocyamine), which is a metabolite of taurine, showed its antagonism at the q1 GABA c receptor [16]. Therefore, taurine and its metabolites may avoid myopia progression as an antagonist of the GABA c receptors.
Second, the release of dopamine diminishes the induction of ocular axial enlargement and taurine showed a synergistic effect with dopamine in the brain [17]. As the retina is an extension of the central nervous system we could potentially infer the same mechanism would be applied. Third, taurine is a potent antioxidant. It reduces the production of reactive oxygen species [5]. Because it increases antioxidant enzyme levels and acts as a free radical scavenger in different tissues (neuronal cells, liver, cardiomyocytes, skeletal muscle, and chondrocytes) [18]. A randomized study of 69 children with Crocetin, another antioxidant, vs placebo showed that Crocetin could significantly avoid myopia progression [19].
Evaluated the protective effect of intravitreal injection of taurine in rats against the toxic effect of N-Methyl-Aspartate, NMDA- induced (a subtype of glutamate receptors) by measuring antioxidant enzyme levels, retinal morphology, and cell apoptosis. They only found in the retina of rats pre-treated with taurine, a significant increase of: superoxide dismutase, retinal glutathione, and catalase [12]. Also, Nor Arfuzir et al. investigated in rats, taurine’s neuroproperties against endothelin 1, a potent vasoconstrictor [9]. The ones treated with taurine demonstrated a significant improvement in production of antioxidant enzymes: retinal glutathione, catalase, and malonil dialdehido, as well as less number of apoptotic retinal cells. An increase in the antioxidant enzyme levels is the best way to demonstrate its antioxidant properties. Overall, those studies showed that taurine, a potent antioxidant, may play a role against retinal degeneration and ocular growth regulator.
Figure: 2 shows a posterior staphyloma of the AO as well as an active CNV of the OI before the treatment with taurine and Anti- VEGF, which after 7 years remained inactive while the patient took taurine 500 mg daily and the OD never developed it. This is a relatively common complication of pathological myopia. Since a new CNV can appear in the other eye up to 35% of patients within 8 years of onset, and showed taurine reduced levels of vascular endothelial growth factor (VEGF), taurine may have avoided the reactivation (OI) or appearance (OD) of CNV in our patient [5,20].
At the last ophthalmological consult, the patient underwent peripheral retinal photocoagulation AO and the visual acuity of the OS severely decreased. Although the patient was treated with corticosteroids, her vision and inflammation improved only slightly, but both recovered 3 weeks after she increased the dose of taurine. Five weeks after, her visual acuity improved even more than one year before. (Table 1)
Furthermore, the anti-inflammatory effect was demonstrated in many reports described a study of induced traumatic brain injury in rats where one week treatment with taurine reduced many cytokines, interleukins (IL-1α, IL-1β, IL-4, IL-5, IL-6, IL10, IL-12p70, IL-13, IL-17), tumor necrosis factor (TNF) - α, among other pro-inflammatory substances [5]. In the study of the rats treated with taurine had retinas with a significantly greater fractional thickness of ganglion cell layer and cell density in inner retina compared to untreated rats, which suggests the neuroprotective effect of taurine [12]. Since inflammation plays a role in pathological myopia taurine may have protected the retina of our patient [20].
Brain and retina are part of central nervous system, so that we hypothesize that taurine helped to decrease the frequency and intensity of the patient’s migraines, despite the dietary parameters previous mentioned, but its mechanism of action remains unknown [7]. Concluded that “taurine plays an important role in brain development, including neuronal proliferation, stem cell proliferation, and differentiation, via several mechanisms”. The use of taurine in migraines is a topic that should be studied because it could bring a new insight to this common health problem.
The effect of higher taurine level to control of myopia needs evaluation. Currently, the patient is taking 500 mg twice a day. Taurine has been used as a treatment: for overweight at 500-1500 mg daily for a year, and for Diabetes Mellitus at 1.5 g daily for 8 weeks without harmful effects [1]. The European food safety authority established the NOAEL (not observed Adverse Effect Level) in 1000 mg/daily [5].
Taurine may have more benefits than adverse effects, which are fatty liver and osteopenia [5]. The patient has only presented osteopenia for the last 2 years and she began taking 600 g/daily of calcium. Furthermore it has been found that taurine has a beneficial effect on bone mass by avoiding osteocyte apoptosis, and may modulate genes to maintain bone homeostasis and regulate bone formation [18]. Therefore, we believe the patient has osteopenia due to other causes different to taurine.
Our case has some limitations. First, a case report study limits generalizability of results. A lack of control group not only increases the probability of confounders and bias but also limits the possibility to establish causality. However, the reported findings may be a first step to evaluate of taurine properties in larger studies. Second, little is known about the appropriate dosing for taurine supplementation.
Our report demonstrates that a dose of 500 mg day could be beneficial in myopia progression without side effects. Third, the patient had a restricted diet (i.e., avoiding dark food) and received other treatments (i.e., anti-VEGF, corticosteroids, vitamins, minerals) during this timeframe which could have also contributed to her vision improvement. Therefore, we consider that controlled randomized studies are needed to identify the potential benefits of taurine supplementation in the management of high myopia.
Although, taurine by itself has not been proved to control myopia progression or to prevent pathological myopia in randomized studies, this case report offers an opportunity to explore in more detail its neuroprotective properties. Also, it allows the generation of hypothesis regarding its use as a coadjuvant treatment in high myopia, and even in migraines. The patient did not present adverse effects in 7 years of taurine use suggesting that it may have a safe profile as a nutritional supplement.
Daily taurine supplementation may have a benefit on myopia progression by controlling the growth of the ocular globe; avoid retinal degeneration; and avoid appearance or reactivation of a choroidal neovascular membrane, probably due to its anti- inflammatory and antioxidant effects. Large clinical studies are needed to evaluate its safety profile and its dose-response effect in high myopia and pathological myopia.
Taurine may also help in migraine control.
We thank Dr. Alejandra Vásquez Ávila for her collaboration on the review and comments that substantially improved the paper.