Author(s): Akshita Panwar*, Kusum Lata, Anurag Khaitan, Isha Kriplani and Alka Kriplani
Significant spontaneous bladder trauma at vaginal birth is rare and affects <1% of deliveries. Bladder contusion resulting in urinary retention 5 days after normal delivery is being described here in a 23-year-old primiparous lady who underwent cystoscopic fulguration of the bleeder. Early diagnosis and prompt treatment can prevent long term, irreversible damage to the detrusor muscle that can have a permanent impact on a woman’s quality of life. A multidisciplinary surgical team comprising gynaecologists, urologists and anaesthetists carried out examination under anaesthesia and cystoscopy. An arterial bleeder below the interureteric ridge in the area of bladder neck was identified and coagulated with Resectoscope loop to secure hemostasis ensuring a safe distance from both ureteric orifices. Postoperative continuous bladder drainage for 3 weeks resulted in complete recovery. Careful evaluation of the stable patient with radiologic imaging and endoscopic management in competent hands should be considered before proceeding with any open surgical procedure in such cases
A 23 years old primiparous lady presented to the emergency department with a self-retaining catheter in situ for urinary retention with hematuria following an otherwise uneventful full term vaginal birth 5 days ago at a private facility. There was history of passing blood mixed urine for the initial 4 days after childbirth and complete urinary retention on the 5th day. A local clinician referred her to our tertiary care centre after catheterisation which drained frank blood. On arrival, she had intense pallor, pulse rate of 110/min, blood pressure of 130/80 and an abdomino-pelvic mass reaching up to umbilicus (Figure 1).

Figure 1: Preoperative picture of abdomen showing well defined abdominal lump approximately corresponding to 24 weeks uterus size.
The urobag contained 300cc of blood mixed urine. A non-bleeding second degree perineal tear was present and on speculum vaginal evaluation, minimal lochia was visible. Vaginal examination revealed normal bleeding with pulled up the a cervix high up and a 20 weeks size well contracted puerperal uterus. Initial resuscitation was done with oxygen, intravenous crystalloids and packed red cells. Haematological evaluation revealed a haemoglobin of 6.9 g/ dl, and normal coagulation profile, liver and renal function tests. An ultrasonography of the pelvis reported suspected urinary bladder injury. CT urography suggested possibility of bladder neck injury in an otherwise intact urinary bladder, a large (10.4x11.3x11.7 cm) haematoma occupying the lower part of bladder lumen with urine in the upper part of the distended bladder with a possible active bleeder at the bladder neck (Figure 2). A small hyper-enhancing vessel was also seen along the posterior wall of bladder on the left side in the region of hematoma with contrast extravasation, not seen on venous phase likely to be a bleeder. (Figure 3). A bulky puerperal abdominal uterus and normal ovaries were also evident.
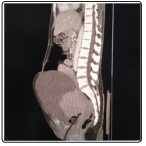
Figure 2: CECT abdomen with pelvis sagittal section showing distended bladder filled with hyperdense blood clots10.4x11.3x11.7cm in the region of neck and trigone surrounding the foley’s catheter balloon and tip. Hypointense contents over the clots suggesting the urine retention. Uterus is seen pulled up behind the bladder.

Figure 3: Cystoscopic image showing superficial injury at the bladder neck after fulguration of the bleeder achieved hemostasis. (Unipolar loop is also seen)
Variable degree of trauma to the urinary bladder may occur in women with prolonged or obstructed labour which in turn is more likely in cases of contracted/borderline pelvis, good sized baby, difficult forceps delivery and neglected labour, though the incidence has come down in recent times with more liberal use of caesarean section [1].Spontaneous or idiopathic bladder injuries occur in less than 1% of all cases and only a few cases have been reported after labor and none during the antenatal period [2].The presentation may range from haematuria to vesicovaginal fistula and rarely may cause life threatening bladder haemorrhage [3].
During labour, bladder neck is placed at a vulnerable position between the symphysis pubis and the fetal head for a variable period of time. This, if prolonged, predisposes to vascular compression and occlusion and ischaemic necrosis of the area with its attendant consequences. The vascular injury in the present case probably occurred during late and prolonged labour and a full bladder at that time may have aggravated the condition. However, there is no method of objective assessment of this trauma that can quantify the degree of injury and the evaluation and management remains primarily clinical. Predisposed women may be encouraged to void frequently during labour, a suprapubic bulge may be looked for and if present should be evacuated by a self retaining catheter till childbirth. Presence of haematuria signifies a higher degree of bladder injury and warrants immediate continuous bladder drainage during and after labour. More often, the intrapartum bladder trauma presents a few days or a week after childbirth if bladder rest was not provided, as occurred in our case. The haemorrhagic urine may be taken as lochial bleeding by an uncatheterised and unwarned patient. Accumulation of heavy blood clots in the lower part of bladder and urine in the upper part ultimately results in urinary retention as happened in this case. There are only a few reports in literature of frank bladder haemorrhage after vaginal birth that required surgical management and this, to the best of our knowledge is the first report of cystoscopic management of such a case. Cystoscopic management should be the procedure of choice for management of a stable patient with active lower urinary tract traumatic vascular aetiology although this procedure may be limited by availability of skill and infrastructure especially in peripheral small health facilities. However, in life threatening situations consequent on massive and partly concealed urinary bladder haemorrhage, an open surgical approach may be better for immediate identification and ligation/cauterisation of the traumatized vessel. The need for multidisciplinary management of such cases cannot be underestimated. Cystoscopic evaluation and multidisciplinary involvement should form an integral part of management of all cases of significant lower urinary tract haemorrhage after a vaginal birth. Early diagnosis and prompt treatment can prevent long term, irreversible damage to the detrusor muscle that can have a permanent impact on a woman’s quality of life.
We appreciate the help of my colleague Dr. Shantanu Singh Tomar.
We have no financial disclosures.