Author(s): Soraya Dendouga
Introduction: The restoration of teeth with composite ceramic veneers has always been a subject of controversy: for some authors the presence of such restorations is a source of failure while for others not necessarily.
Material and Method: Our study; is a randomized clinical trial comparing three types of crown preparations for bonded ceramic veneers.
Our clinical trial which evaluated 264 bonded veneers in 73 patients included 235 living teeth and 29 mortified teeth that underwent endodontic treatment. Among the secondary objectives of this study: the evaluation of the durability of ceramic veneers bonded to teeth with composite restorations.
Results: The Chi-square test of the occurrence of events according to the unblocked / blocked character gives a p = 0.05 (p ≤ 0.05) so the difference is significant.
Conclusion: The presence of composite fillings affected the survival rate of veneers in our study.
In a society concerned with aesthetics, patient demand more frequently directs us to restorations invisible to their eyes. Adhesive dentistry has been able to respond not only to these growing aesthetic requirements but also to the continuing desire of practitioners to be as minimally mutilating as possible in their practice.
Among the aspects of this dentistry, ceramic veneers occupy an important place. This technique, which has become widely accepted in recent years, has given rise to the reflection of several researchers: preparation techniques, ceramic materials and glues; have been evaluated in different clinical and laboratory studies. We conducted a randomized clinical trial which focused on the comparison of the different types of coronary preparations (main objective). Among the secondary objectives of this trial was to know if the presence of composite fillings on the abutment teeth was a determining factor for the durability of ceramic veneers.
The subjects are recruited from among those who come to the dental prosthesis service at the Mustapha university hospital in Algiers.
The diagnosis of anomaly; color ; form ; minor structure or malposition will be objectified to the naked eye during clinical examination.
Subjects comparable by one of the anomalies cited and diagnosed will be treated by one of the techniques determined by random draw.
Any anterior tooth with:
typical color abnormality: amelogenesis imperfecta due to
tetracyclines; fluorosis; colorings due to age, coloring of external
origin (tea, coffee or tobacco) by infiltration of the tissues; teeth
discolored without loss of substance;
An anomaly of form: microdontia; atypical form case of conoid
incisors;
An anomaly of structure or texture: dysplasia, dystrophy, erosion,
attrition, mechanical or chemical abrasion and coronary fracture;
A minor rotational malposition.
Our study will concern both men and women, but whatever the
case, we will only include patients deemed reliable, cooperative
and likely to be monitored regularly
General condition: healthy patient with no general or local
pathology;
Oral hygiene: must be satisfactory;
Type of teeth: to reduce the variations, we will limit ourselves to
the incisor-canine block.
Criteria
We will not include in our study anyone:
Deemed unable to understand the essay, uncooperative or unstable.
With a contraindication to glued ceramic veneers, namely:
Aged teeth;
Abrasive teeth;
Presence of parafunctions;
Unfavorable occlusal relationships;
Poor oral hygiene.
Methods
Type of Study
Our study is a randomized clinical trial comparing three types of
crown preparations for bonded ceramic veneers.
During this trial the allocation to the different treatment groups is
done at random, by drawing lots, thus ensuring the comparability
of these groups.
The same operator will proceed to the draw as follows:
? The distribution in all the different groups will be based on
chance;
? We are dealing with two variables the teeth (central, lateral,
canine) and the type of preparation (type I, II, III);
Dental Preparation Method for Ceramic Veneers
It differs from conventional preparations in that the retention of
the prosthetic element is only ensured by bonding.
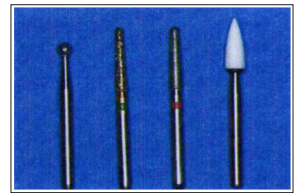
*Material Needed for Preparation
The preparation protocols use the concept of controlled tissue
penetration through the use of diamond burs calibrated for this
purpose.
Several authors have proposed several boxes. Among these authors Bernard Touati, and Galip Gurel.
A set of 3 strawberries is sufficient for a good preparation.
Diamond round bur which delimits the desired indentation in
the dentin;
Fillet bur which eliminates grooves and marks the cervical limit:
Red ring cutter: fine grain for finishing.
Preparation Methods
Our study is a randomized clinical trial comparing three types of
crown preparations for bonded ceramic veneers.
During this trial the allocation to the different treatment groups is done at random, by drawing lots, thus ensuring the comparability of these groups.
The same operator will proceed to the draw as follows: The allocation to all the different groups will be based on chance;
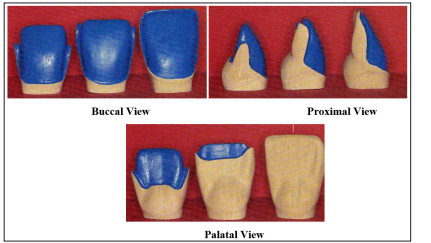
Figure 2: The Three Types of Preparation for Ceramic Veneers on Maxillary Anterior Teeth [1,2].
From left to right preparation in semi-jacket; preparation in slight return; preparation without palatal return.
*Technique for Making Coronary Preparations
To avoid production bias, all of the clinical steps for the ceramic
veneers performed in the study (dental preparation, bonding and
control) were performed by the same practitioner.
The ceramic veneers were fabricated by a single prosthetist who used the same technique and the same low-melting ceramic (Finesse® All-Ceramic, Ceramco; U.S.A)
All veneers were bonded with Variolink II® (Variolink II, Ivoclar Vivadent, lot no M10683, lot n° M34435, lot n° P22457), a dual curing composite prepared according to the manufacturer’s instructions
Control Sessions
Patients are invited to follow-up sessions after: 6 months, 12
months, 24 months, 36 months, 48 months and 60 months.
During these appointments, the veneers were visually inspected and evaluated according to the criteria studied.
Clinical Case
An 18-year-old female patient consulted for improvement of her
smile: Dean’s type II dental fluorosis. This well-informed patient
requested ceramic veneer treatment.
Before this stage of fluorosis, prosthetic restoration is the rule and ceramic veneers represent the most conservative form.
Clinical examination revealed:
Dean’s Class II dental fluorosis
An agenesis of the 13 parallel to a 22 which is small.
An irregularity of the levels of the collars.
A non-gingival smile: full lips

Figure 3: Initial Situation
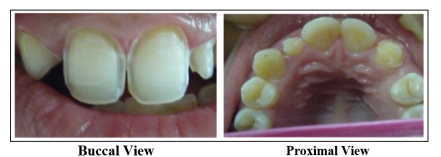
Figure 4: Coronary Preparation

Figure 5: Final Result After Gluing the Veneers
The 13 transformed into lateral: only a preparation with incisal overlap could make this possible.A better aesthetic result could have been obtained in association with periodontal surgery which would aim to correct the alignment of the necks.
The full lips and the non-gingival smile observed in the patient made it possible to alleviate this problem.
The mean age of patients at the start of treatment was 27 years with a range of 13 to 49 years.
The number of veneers varies from “one” to “six” per patient. All veneers were performed at the level of the upper anterior block.
Once the treatment is finished, patients are invited to come back if there is a problem with their veneers or abutment teeth. Patients will be checked after 6 months; 12 months ; 24 months; 36 months; 48 months; 60 months. The information collected during these checks is reported on the clinical sheet.
All the patients participated in the various controls, only one patient, who benefited from two restorations at the power plants did not participate in the study and this from the second booster (12 months), which is equivalent to a rate abandonment or loss of follow-up in 1.40% of patients (0.76% of restorations).
Descriptive Study
Distribution of the Population by Sex
Table 1: Distribution of Patients by Sex
| Sex | Effective | Percentage |
|---|---|---|
| Feminine | 52 | 71,23 % |
| Male | 21 | 28,76 % |
| Total | 73 | 100,00 % |
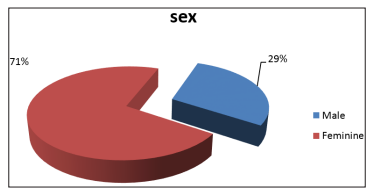
Figure 6: Distribution of Patients by Sex
The sample studied shows a predominance of the female sex with a number of 52 women among 73 patients, which represents 71.23% of the total number. The male sex, numbering 21 men, has a frequency of 28.76%.
Distribution of the Population by Age
Our population includes patients aged 13 to 49 years. The age
groups are broken down as follows:
Table 2: Distribution of Patients by Age
| Age group (year) | Effective |
|---|---|
| [12, 14[ | 01 |
| [14, 16[ | 02 |
| [16, 18[ | 01 |
| [18, 20[ | 05 |
| [20, 22[ | 06 |
| [22, 24[ | 09 |
| [24, 26[ | 07 |
| [26, 28[ | 09 |
| [28, 30[ | 08 |
| [30, 32[ | 05 |
| [32, 34[ | 03 |
| [34, 36[ | 07 |
| [36, 38[ | 02 |
| [38, 40[ | 02 |
| [40, 42[ | 01 |
| [42, 44[ | 01 |
| [44, 46[ | 02 |
| [46, 48[ | 01 |
| [48, 50[ | 01 |
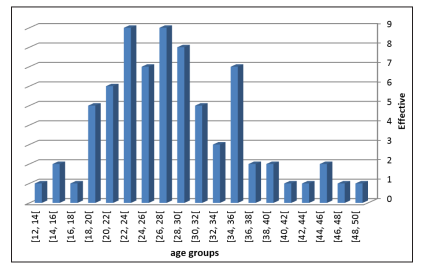
Figure 7: Distribution of Patients by Age
The average age of our study population is 27.71 years; (95% CI = [25.90 years; 29.52 years]). The median age of the sample is 27 years with a minimum age of 13 and maximum age of 49.
? Number of Veneers Depending on the Type of Prepared Tooth
Table 3: Number of Veneers by Type of Prepared Tooth
| Type of tooth | Numbers | Percentage |
|---|---|---|
| Central incisor | 120 | 45,45 % |
| lateral incisor | 86 | 32,58 % |
| Canine | 58 | 21,97 % |
| Total | 264 | 100,00 % |
120 central incisors (11 and 21) were treated with ceramic veneers, which represent 45.45% of all facets. 32.58% represents the percentage of lateral treated veneers while the canines represent only 21.97% of the whole.
? Distribution of Veneers According to the Character of the Non-Filled Tooth / Filled Tooth
Table 4: Frequency of Veneers According to the Character of the Tooth Not Filled / Filled Tooth
| Dent pilier | Effective | Pourcentage |
|---|---|---|
| non-obturated | 208 | 78,79 % |
| obturated | 56 | 21,21 % |
| Total | 264 | 100,00 % |
The veneers were bonded to 208 non-filled teeth, corresponding to 78.79% of all teeth, while 56 of the veneers were bonded to filled teeth, or 21.21%.
| Characteristics of the tooth | Crack, fracture, detachment,pulpitis, abutment toothfracture | Total | |
|---|---|---|---|
| No | yes | ||
| Not obtured | 199 | 9 | 208 |
| 95,67% | 4,33% | 100,00% | |
| Obtured | 46 | 10 | 56 |
| 82,14% | 17,86% | 100,00% | |
| Total | 245 | 19 | 264 |
| 92,80% | 7,20% | 100,00% | |
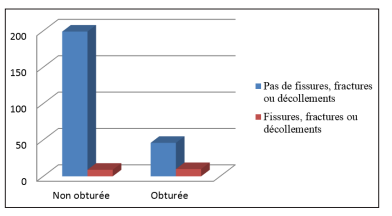
Figure 8: Histogram of the Occurrence of Cracks, Fractures, Detachments According to the Character of the Filled Tooth / Non-Filled Tooth
The occurrence of cracks, fractures, facet detachments was observed with a percentage of 4.33% on the non-filled teeth and in 17.86% of the filled teeth.
Distribution of the Type of Preparation According to the Composite Fillings
Table 6: Frequency of Preparation Type According to Composite Fillings| Type depréparation dentaire | compositefilling | Effective | Percentage |
|---|---|---|---|
| Type I | Absence | 72 | 82,80% |
| Présence | 15 | 17,20% | |
| Total | 87 | 100,00% | |
| Type II | Absence | 73 | 79,30% |
| Présence | 19 | 20,70% | |
| Total | 92 | 100,00% | |
| Type III | Absence | 66 | 77,60% |
| Présence | 19 | 22,40% | |
| Total | 85 | 100,00% |
Composite filling is an important consideration when dealing with ceramic veneer restorations.
The three types of preparation were carried out mainly on teeth which did not present composite fillings: type I at 82.80%; type II at 79.30% and type III at 77.60%.
Distribution of the Occurrence of Cracks, Fractures, Detachments, Pulpitis, Abutment Tooth Fractures According to the Non-Obturated / Obturated Nature.
Table 7: Frequency of the Occurrence of Cracks, Fractures, Detachments, Pulpitis, Abutment Tooth Fractures According to the Non-Obturated / Obturated Character
| Caractéristiques de la dent | Crack, fracture, detachment, | Total | |
|---|---|---|---|
| Non | Oui | ||
| Not obtured | 199 | 9 | 208 |
| 95,67% | 4,33% | 100,00% | |
| obtured | 46 | 10 | 56 |
| 82,14% | 17,86% | 100,00% | |
| Total | 245 | 19 | 264 |
| 92,80% | 7,20% | 100,00% | |
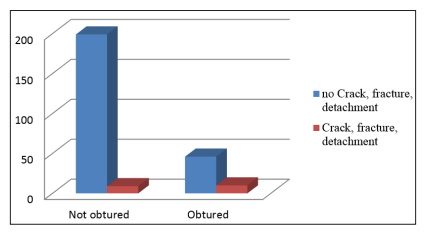
Figure 9: Histogram of the Occurrence of Cracks, Fractures, Detachments According to the Character of the Filled Tooth / Non-Filled Tooth
The occurrence of cracks, fractures, facet detachments was observed with a percentage of 4.33% on the non-filled teeth and in 17.86% of the filled teeth.
Analytical Study
Although Kaplan-Meier statistics were originally designed to deal
with individuals, the use of the tooth as a statistical unit instead
of the person is justified [3].
In the present study, the Kaplan-Meier analysis was done in two
different ways: the first analysis is related to the patient, the second
was performed using the restoration as the statistical unit.
Our study is a clinical trial where we seek to evaluate the
effectiveness of one type of preparation compared to two other
types and this by comparing the results obtained in each group.
Faced with a difference observed between the groups, there are
two possibilities either this difference is due solely to chance, or
this observed difference is real.
We applied the “Chi2” test to check the dependence or not
between the variables and the different groups. This probability
is called “p”. The p-value is the threshold from which the observed
difference is considered to be statistically significant. This means
that it is real and has a low chance of being due to chance.
When p is ? 0.05 the difference is significant
When p is> 0.05 the difference is not significant.
Veneer Survival Rate According to the Character of the Tooth not Filled / Tooth Filled

Figure 10: Survival Curve of Ceramic Veneers According to Character (closed / unblocked)
The survival rate of unblocked teeth is 96.20% (95% CI; [93.70%; 98.80%]) with an average survival time of 59.20 months (95% CI; [57.95 months; 60.45 months]).
The survival rate on filled teeth is 87.60% (95% CI; [78.70%; 97.50%]) with an average survival time of 58.33 months (95% CI; [54.00 months; 62.66 months]).
The overall survival rate of ceramic veneers according to the “unblocked / closed” criterion is 90% with an average survival time of 53.33 months (95% CI; [54.00 months; 62.66 months]). The Log-rank test for the occurrence of events according to the healthy / mortified character gives a p = 0.05 and therefore the difference is significant.
Therefore, the presence of composite fillings may have an impact on the survival rate of the veneers in our study.
Discussion
Our study; is a randomized clinical trial comparing three types of
crown preparations for bonded ceramic veneers.
We are interested in the role that the design of the coronary
preparation can play on the longevity of ceramic veneers.
These restorations, whose translucency meets current aesthetic
requirements, are increasingly in demand, but little information,
little clinical work is available on this subject.
Our population size includes 73 patients. Analysis of our sample shows a predominance of the female sex with a number of 52 women representing 71.23% of the total workforce and 21 men representing 28.76%.
This predominance of the female sex is explained by the fact that women are more concerned about their appearance than men. They are aware of the role that a beautiful smile can play. Well informed, they demand not only aesthetics but also the least mutilating possible size of their teeth.
Our results are in agreement with the study carried out by Dumfabrt Herbert where the majority of patients were female (60%). It also confirms that these results have been reported in other clinical evaluations on ceramic veneers.
The average age of our study population is 27.71 years. The median age of the sample is 27 years with a minimum age of 13 and maximum age of 49.
This is a young population: at this age group, patients are very concerned about their appearance, which the study by Hamzawi- Decharrière et al. (2007) where they announced that aesthetic demand over the next five years will represent 60% of the reasons for consultation, especially among young patients.
Impact of Composite Fillings on the Survival of Ceramic Veneers
In our study, 264 teeth were restored with ceramic veneers: 208 non-filled and 56 filled teeth: The survival rate of unblocked teeth is 96.20% (95% CI; [93.70%; 98.80%]) with an average survival time of 59.20 months (95% CI; [57.95 months; 60.45 months]
The survival rate on filled teeth is 87.60% (95% CI; [78.70%; 97.50%]). with an average survival time of 58.33 months (95% CI; [54.00 months; 62.66 months]);
The overall survival rate for ceramic veneers according to the “unblocked / filled” criterion is 90% with an average survival time of 53.33 months (95% CI; [54.00 months; 62.66 months] ).
The Chi-square test of the occurrence of events according to the unobstructed / obturated character gives a p = 0.05 (p ? 0.05) so the difference is significant: the presence of composite fillings has an impact on the rate of facet survival in our study. In the documentation consulted; Although investigators evaluated the effect of the design of the ceramic veneer preparation, little information is available regarding the design of the preparation in association with the condition of the existing tooth structure. Among the risk factors for a higher number of premature loss of ceramic veneers, as mentioned in the literature, the presence of fillings on the teeth concerned (Dunne & Millar 1993; Shaini et al. 1997), a significant loss of hard dental tissue existing before the start of veneer treatment (Dunne & Millar 1993) [4]. In the articles consulted we find that: Calamita M. A in a retrospective study concluded that among the 42 failures, only 3 occurred at the level of the teeth with restorations, and no significant association could be observed between the failure and the presence of a restoration [5].
Dumfahrt and Schaffer (2000) by analyzing 205 ceramic veneers in 72 patients concluded that the failure rate increased (p <0.01) when the finish line crossed an existing filling and (p = 0.058) when parts of the preparation surface were in the dentin. The weak link in the veneer bond was considered the dentin / glue bond [3]. Guessa P. C, Stappert C. F.J (2008) state that the presence of composite fillings cannot increase the loss of veneers in their study, they even had a negative impact on the overall clinical performance. At the underlying vulnerable ceramic / tooth / composite interfaces, strong marginal discoloration was noted in 12 restorations [3,6,7].
They explain this by the presence of gaps in the physico-mechanical properties of the composite resin, such as polymerization shrinkage, elasticity, high coefficient of thermal expansion and limited wear resistance. On the other hand, the bond of the ceramic to the composite restoration is inferior compared to the bond to enamel or dentin. Finally, the high thermal expansion (inter-proximal) of composites has a negative influence on marginal adaptation. During large temperature changes, the contraction and expansion of composites results in tensile and compressive stresses at the edge of the ceramic veneers with loss of bond, deformation of the veneer margins and the formation of cracks as a result. Thermal stresses can be minimized by partially or fully encompassing pre-existing composite restorations.
Karlsson (1992) reports that the presence of composite seems to increase the risk of infiltration. In addition the connection of the composite to the dentin; at the restoration-dentin interface, may be the weakest link Murphy et al. (2005) in a 5-year retrospective evaluation that included 29 patients, 62 veneers reported a correlation between failure and the presence of pre-existing composite restorations [3].
Peumans et al. (2004) in their clinical study on the evaluation of the clinical performance of ceramic veneers after 5 and 10 years of clinical service and knowing that fillings were present in 70% of the ceramic veneers in their study; reported that the presence of composite does not appear to influence veneer retention even after 10 years. They explained this in part by the in vitro results of Magne et al. which showed that respect for the original tooth in fractured teeth was almost restored when the composite was used to replace the missing dentin, with the ceramic acting only as a substitute for the enamel [7,8,9,].
Shaini F.J; Shortanll A.C.C; Marquis P.M observed increased failure rates and the development of problems when ceramic veneers were bonded to existing composite restorations [10]. In addition, a numerical study has shown that the partial or total envelopment of composite fillings is indicated to minimize thermal stresses. With medium or long type ceramic proximal wraps, part of the composite volume is replaced by ceramic, which decreases the influence of expansion or contraction of the underlying composite filling [11].
A study done in 1991. This study investigated a load applied to a bonded veneer to the tooth, where the underlying incisal edge is either a bonded fragment, a composite restoration, or the intact tooth. The force at which the break occurs in the facet; as seen in the tooth as well, depends on its flexural strength, the modulus of elasticity of the underlying material, the dimensions and the strength of the bonds between the materials. She reported in contrast, a significantly higher tensile strength in the absence of initial treatment and the fractured incisal edge was restored with a layered veneer. The fracture resistance of the veneered restoration directly on the fractured tooth was not different from that of intact teeth restored with veneers [12].
Then in study Magne and Douglas evaluate the distribution of the stresses for teeth presenting coronary fractures. These teeth were divided into two groups: teeth restored with ceramic veneers after composite reconstruction, and teeth restored with ceramic veneers only. The results show that the prior restoration of decayed teeth is a technique ensuring better flexibility. Another study shows that the resistance to fracture of ceramic is influenced by the modulus of elasticity of the material used for the reconstruction [13,14].
Our results are in agreement with those of Dunne & Millar 1993, Dumfahrt and Schaffer (2000); Murphy et al. (2005) ; Shaini et al. 1997 [15,16,17].
In our study, the influence of composite restorations on the longevity of ceramic veneers can be explained by the physico-mechanical properties of the composite resin which have shortcomings, such as polymerization shrinkage, elasticity, coefficient of thermal expansion high and limited wear resistance. When ceramic is applied to enamel, the more rigid substrate absorbs the stress due to the function and prevents the ceramic from fracturing. Conversely, when ceramic is applied to the composite resin, the stress will be absorbed by ceramic which will fracture due to its fragile nature.
On the other hand, the bond of the ceramic to the composite restoration is weaker compared to the bond to enamel or dentin. The high thermal expansion of composites has a negative influence on the marginal fit. During large temperature changes, the contraction and expansion of composites results in tensile and compressive stresses on the margins of the ceramic veneers with loss of bond, deformation of the facet margins and the formation of cracks as a result. Thermal stresses can be minimized by partially or fully encompassing pre-existing composite restorations.
Conclusion
Within the methodological limits of our clinical trial which
evaluated 264 veneers placed in 73 patients (52 women and 21
men) of an age range ranging from 13 years to 49 years with an
average age of 27.71 years and after 64 months of follow-up (5
years and 4 months), the presence of composite restorations is a
risk factor for the production of ceramic veneers.
References