Author(s): Udaya M Kabadi* and Sarah Exley
American college of Obstetrics and Gynecology recommends 2 step testing at 24-28 weeks or earlier if indicated by symptoms; 1. determination of plasma glucose at 1 hour following ingestion of glucose liquid 50 g at any time of the day irrespective of the prior meal. 2. If plasma glucose is > 140 mg/dl, Oral glucose tolerance test for 3 hours following ingestion of glucose 100 g after an overnight fast on a separate day [1]. Alternatively, American Diabetes association recommends 1 step testing; 2 hour oral glucose tolerance test following ingestion of glucose liquid 75 g after an overnight fast [2]. Thus, both present screening tests for gestational diabetes, by either ACOG or ADA involve ingestion of liquid glucose. Moreover, both step 2 OGTT recommended by ACOG and OGTT approved by ADA require 3 day preparation with least daily intake of carbohydrate 150g for 3 days prior to testing [1,2]. Moreover, many women report nausea and some even vomiting in response to ingestion of glucose liquid and shun preparation as well and therefore are hesitant to get tested. Herein we report a successful use of serum fructosamine as a screening test in eliminating diagnosis of GDM confirmed by a simultaneous continuous home blood glucose monitoring for 10 days.
37-year-old Caucasian woman (AH) was seen in endocrine clinic for a routine follow up visit for monitoring of primary hypothyroidism and pregnancy at 24 weeks. Her obstetrician is observing her closely because of pregnancy induced by in vitro fertilization. She did not have GDM during her previous pregnancy also induced by in vitro fertilization and the new born had weighed 7lb and 11 oz. Attempt was made to administer glucose liquid 50 g. orally as the 1st step testing for gestational diabetes. Unfortunately, she developed nausea followed by incessant vomiting and the test was promptly terminated. She therefore declined to repeat the same test because of a concern about nausea and vomiting caused by glucose liquid. She inquired of me if any other test could be conducted to assess the presence of GDM. I recommended hemoglobin A1C since it is recommended by ADA as a diagnostic test in nonpregnant adults [2]. Moreover, A1C is a marker of average blood sugar over 3 months’ duration and she was 24 weeks pregnant. I also recommended serum fructosamine level as it denotes average blood glucose over three weeks’ period [3]. However, the obstetrician suggested that we perform continuous glucose monitoring for 10 days to establish diagnosis
Blood was withdrawn in the endocrine clinic and was sent immediately to local laboratory for determination of HbA1c and serum fructosamine concentrations to assess presence of GDM. Serum Free T4 and TSH concentrations were also determined to assess adequacy of levothyroxine dose in management of primary hypothyroidism. All tests were performed by the local laboratory with established assays, CGMS device (Freestyle Libre by Abbot Laboratories, Abbot Park, Illinois) was applied to the lateral side of the upper arm for continuous glucose monitoring lasting 10 days. She reported to clinic at day 11 for down load of CGMS.
HbA1c as well as Serum fructosamine Fasting plasma glucose , free T4 and TSH were all within the normal and desirable ranges (Table 1). CGMS showed normal blood sugars throughout the day including morning after an overnight fast as well as both pre and post prandial periods. (Figure 1)
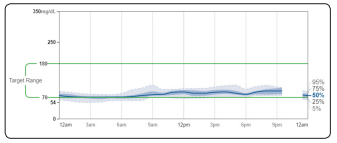
Figure 1: Daily Average Ambulatory Glucose Profile with Continuous Glucose Monitoring over 10 days
Table 1: Fasting plasma Glucose (mg/dl), HbA1c (%) and Fructosamine Levels in Subject AH and Reference Range
| Fasting Plasma Glucose mg/dl | HbA1C % | Fructosamine umol/L | |
|---|---|---|---|
| AH | 84 | 4.8 | 192 |
| Range | 65-99 | 4.8-5.7 | 200-285 |
Screening tests for assessment of GDM established by ACOG and ADA are decades old and involve ingestion of liquid glucose and pre testing preparation [1, 2]. Many pregnant women experience vomiting during pregnancy, which is further exacerbated by ingestion of liquid glucose. Moreover, oral glucose tolerance tests are inconvenient and already being replaced in nonpregnant subjects by HbA1c, random or fasting blood glucose as recommended by ADA [2].
This report demonstrates that HbA1c and serum fructosamine levels matched very closely with average blood sugars over 10 days determined by CGMS and excluded the diagnosis of GDM in our subject. Therefore it is apparent that both HbA1C and serum fructosamine may be reliable and accurate in assessment of GDM. Serum fructosamine level may be more sensitive than HbA1c since it denotes average blood sugar over 3 weeks as compared to 3 months for HbA1c(3). Finally, serum fructosamine determination is likely to be more convenient even for repeated testing during pregnancy as it does not require fasting and could be conducted at any time of the day. However, this observation is limited to this preliminary case report. Therefore, a large study is now under way to further examine the utility of HbA1c and serum fructosamine by conducting the comparative analysis between these tests and current 2 step testing recommended by ACOG.