Author(s): O Makoyo Komba*, JA Bang Ntamack, Mpigha Ekambou L, U Minkobame, P Assoumou and JF Meye
The combination of fibroma and pregnancy presents many maternal complications, ranging from simple pelvic pain to digestive, urinary and hemodynamic complications. Fetal complications range from the threat of preterm delivery to fetal loss. Management is usually surgical and termination of pregnancy may be indicated. We report the case of a 35-year-old nulliparous pregnant woman, within her 18th week of amenorrhea, who presented to us with a picture of profoundly altered general condition following compressive complications from a giant uterine fibroma.
Uterine fibroids are a very common pathology in women of childbearing age [1]. When they reach large dimensions, fibroids cause compression of surrounding organs and are the cause of serious complications. Giant uterine fibroma during pregnancy is a rare, usually symptomatic condition that is not always easy to diagnose [2].
The management of these giant fibroids and the successful completion of the pregnancy at term are sometimes a real challenge for the gynecologist where the surgical option is often preferred, but must take into account the preservation of fertility [3]. When the mother’s life-threatening prognosis, termination of pregnancy and radical surgical treatment may be the only alternative.
We report a rare case of a giant fibroid in a polymyomatous uterus from a pregnant woman within her 18 weeks of amenorrhea in a 35-year-old nulliparous, cachectic subject. To our scrutiny, the termination of pregnancy and the hysterectomy were irremediable.
Mrs. K.M, 35 years old, primigest and nulliparous. Referred to our service because of a severe deterioration of the general condition in the 18th week of amenorrhea pregnant patient presenting an excessive uterine height for this considered term.
In the history of pregnancy, we note that it is a spontaneous pregnancy, desired, correctly followed since it has benefited from 3 prenatal contacts during which it was demonstrated an active monofetal pregnancy developing in sequestration in a polymyomatous uterus carrying a giant submucosal fibroma about a size of 12 cm in length which already presaged the installation of fetal maternal complications during the course of the pregnancy. An early termination of the pregnancy had been suggested with a view to a prior myomectomy, but this attitude was declined by the patient.
The history of the disease provides information on hospitalization a month before, for dyspnea associated with phlebitis of the right lower limb, stopping of intestinal transit, and pollakiuria progressing in a context of severe weight loss.
A patient in very poor general condition, cachectic, undernourished with pale conjunctivae, weighing 45 kg with a body mass index of 17 kg/m² and a loss of 25 kg in five months. She had a blood pressure of 80/60 mmhg, a heart rate of 139 beats/min, and orthopnea. A shiny abdomen increased in volume with collateral venous circulation. A cardboard skin, the uterine height was 40 cm, and dullness on percussion and an indurated mass plunging into the epigastrium and filling the two hypochondria (Photo 1). Significant edemas; lower limbs going up to the inguinal level and taking the cup.

Photo 1: Patient Lying Down
Abdomino-pelvic ultrasound confirmed a large polymyomatous uterus compressing full intra-abdominal organs with a live fetus with 18 weeks of amenorrhea. The ultrasound hardly identified a large heterogeneous calcified intra-abdominal mass but did not determine its origin.
An abdominal pelvic magnetic resonance imaging had been requested showing a large fibroma in the process of necrobiosis measuring 29 x 32 cm, in the sagittal plane with a pedicle of 7 cm. Faced with this picture of dyspnea, severe deterioration in general condition, increased undernutrition, the patient was admitted to intensive care and we decided to terminate the pregnancy for maternal rescue. After failure to induce labor with misoprostol, we opted for surgical management by laparotomy.
During the operation, almost all of the abdominopelvic cavity is occupied by the fibroid (Photo 2), we objectify a large polylobed uterus with a giant sub-serous pedicled myoma (Photo 3). We decide on radical treatment by performing a subtotal, inter-adnexal hysterectomy, en bloc removing the fetus. The pedicled fibroma measured 34 x 32 cm and weighed 9.340 kg (Photo 4), the gravid uterus carrying the other myomatous nuclei measured 27 x 18cm and weighed 3.500 kg, for a total uterine weight of around 13.00 kg.
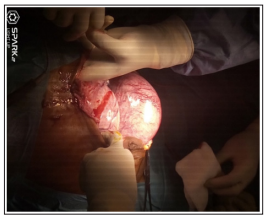
Photo 2: Coeliotomy by Laparotomy; Midline Incision Bypassing the Umbilicus to the Epigastrium.t

Photo 3: polymyomatous uterus and giant pedicled fibroma.

Photo 4: Fibroma of 32 x 34 size.
Histology well confirmed the leiomatous nature without malignancy of the masses. The patient was discharged from the hospital 3 weeks after the surgery.
Uterine leiomyomas are common benign tumors in women of childbearing age [1]. During pregnancy, fibroids increase in size due to increased hormonal impregnation [2]. Giant uterine fibroid during pregnancy is a rare, unusual situation because the myomatous uterus being impacted in different places, implantation and development of the egg can be compromised [4]. Thus submucosal myomas can cause mechanical and vascular endometrial alterations and induce stromal alterations such as atrophy or ulceration reducing the chances of placental development [5].
We were faced with an elderly nulliparous, pregnant after a very long period of unsuccessful search for pregnancy. Hence the stubbornness in carrying this pregnancy to term, despite the indication of myomectomy performed in the first weeks of gestation. The desire for increased motherhood in this patient made the therapeutic decision difficult to make.
Fibroids can grow to large sizes and weigh more than 11.5 kg, diagnosis is not always easy [3,6]. In the case that we describe, the fibroid weighed 9.340 kg. In the case that we describe, the fibroid weighed 9kg 340. We find a varied and rich symptomatology: a significant increase in abdominal volume with a mass effect due to bladder compression (pollakiuria, bilateral hydronephrosis and renal dysfunction), it Associated with this were digestive symptoms such as constipation, and hyporexia due to reduced stomach size , thrombosis of the lower extremities, severe pulmonary hypertension, and respiratory failure that involved the patient. Life-threatening prognosis [7]. This picture of hemodynamic instability evolving on a ground weakened by the pregnancy state. Hence the patient’s admission to the intensive care unit.
1. A terminal AIDS in the face of profound deterioration in general condition and cachexia; 2. A terminal intra-abdominal malignant tumor in front of the uterine volume and cachexia.
This demonstrates the variability of clinical expression and the diagnostic difficulty that can arise with a giant fibroid associated with pregnancy. In fact, fibroids can complicate the course of pregnancy and conversely, being pregnant can facilitate the progression of fibroids to complications [8].
The number of nuclei influences the course of pregnancy in a myomatous uterus, in that 1 in 9 patients with polymyomatous uteri spontaneously aborted compared to 1 in 21 of those with a single nucleus [5]. Had several, of different sizes and locations. This did not stop the progress of the pregnancy. The isthmic localization of certain nuclei acts as a natural girdle or banding and prevents early abortion or the expulsion of the fetus after induction. Indeed, cervical or isthmic myomas interfere with the ampliation and accommodation of the presentation [8].
Preservation of fertility was our starting option with an attempted medical termination of pregnancy followed subsequently by scheduled myomectomy. This alternative ended in failure. the dead fetus being sequestered between the different myomatous nuclei. the opening of the cervix and the expulsion of the fetus could not be completed. The retention of the dead fetus, forced us to perform the laparotomy with the primary aim of lifting the compression and if possible extracting the dead fetus. During the operation, myomectomy seemed unnecessary, the uterus being strewn with several myomatous nuclei and the uterine myometrium is almost absent. This motivated the radical treatment, namely sub-total hysterectomy with conservation of the appendages en bloc, removing the fetus.
The presence of a giant uterine fibroid can make it difficult for a pregnancy to develop. The combination of the two can be fatal for the mother. The pregnancy could not be prolonged because the maternal condition did not allow it. We were unsuccessful in preserving the fertility of this patient, as a myomectomy was impossible due to the non-existence of the non-existent myometrium.