Author(s): Manisha Yadav*, Shilpi K.Pandey, Poonam Agrawal, Devikarani S Khurpade, Ankita Roy and Shubham Bhuktar
Progressive carious and inflammatory involvement of teeth if left untreated will ultimately lead the loss of tooth structure in the oral cavity. Earlier clinician was left with no option but extraction of such hopeless teeth followed by replacement with fixed partial denture, removable partial denture or implants. Hemisection is a removal of compromised root and the associated crown portion. It is one of the treatment options for preserving remaining part of molar having sound periodontium. This case report presents a patient in which distal half of the teeth was carious but with sound periodontium and the periodontally compromised mesial root was resected, and after healing, fixed dental prosthesis was delivered to restore proper form and function
As a practitioner of art and science of dentistry, a clinician is expected to provide a functional dentition for lifetime. Loss of the posterior teeth may result in several undesirable sequelae which requires prevention and maintenance measures. The treatment options for an extensively decayed and unrestorable molar are limited. The most common treatment for such tooth may include extraction followed by a removable partial denture, fixed partial denture, or a dental implant to replace the missing tooth. However, with appropriate case selection, hemisection can be a relatively simple, conservative, inexpensive treatment with good chances of success [1]. Hemisection is a conservative way of preserving tooth. The term “hemi section” or “root amputation” are synonyms for “root sectioning” or “bisection” and is a treatment modality, which allows the preservation of tooth structure, alveolar bone and cost savings over other treatment options [2].
A 35-year-old female patient, reported to the Department of Periodontics in Rungta College of dental science & research bhilai, with the chief complaint of loose tooth and pain in lower left back region of the jaw. Pain was dull aching and intermittent in nature, which aggravated on mastication. On further enquiry, patient did not give any significant medical and previous dental history. Extra oral examination revealed no abnormality. On intraoral examination, tooth #46 had a deep carious lesion involving distal and occlusal surfaces (figure 1). The involved tooth was severely tender on percussion. On probing, a periodontal pocket of 6 mm was found on the mesial aspect with Grade 1 mobility in the affected tooth.
Radiographical examination revealed carious lesion extending to the coronal portion of the distal root. Severe bone loss was observed in the mesial aspect of the root with furcation involvement Interproximal bone loss was evident between #46 and #45 (Figure2). On the basis of history, clinical and radiographic examination, a diagnosis of chronic apical periodontitis was made with respect to tooth #46.Patient was explained about the various treatment option available along with their prognosis including extraction and placement of dental implant. However, she opted for hemisection followed by fixed dental prosthesis over other treatment options.
The periodontal prognosis of the distal root was fair with good bone support. After completion of endodontic treatment that also included removal of all carious tooth structures. (Figure3) Hemisection of mesial root was performed under local anesthesia. Full thickness flaps were elevated on the buccal and lingual aspects of the involved tooth. Upon reflection of the flap, crater like bony defect along the mesial root became more evident. Degranulation was performed using surgical curettes (Hu-Friedy, Chicago, IL,
USA) to expose the bone. A low speed surgical length fissure carbide bur was used under saline irrigation to make vertical cut toward the furcation area. A fine probe was passed through the cut to ensure separation. After completion of the sectioning, the root was elevated from its socket using a periosteal elevator and removed. Granulation tissue was curetted out of the distal socket using surgical curettes. The socket was irrigated adequately with sterile normal saline. Flap was approximated and sutured with 3-0 braided silk. The occlusal table was minimized to redirect the forces along the long axis of the distal root. Immediate postoperative radiograph showed the well-retained distal root and extraction of mesial root (Figure4). At 1-month recall visit, healing was found to be satisfactory, while mobility was absent
Tooth preparation of the distal portion of the first permanent molar and second premolar was performed followed by porcelain-fusedto-metal prosthesis (Figure 5). Final impression was made using putty-reline technique and master cast was obtained. Mandibular master cast was mounted using interocclusal record. Wax pattern was fabricated, sprued, and invested. Casting procedure was carried out using standard techniques. Metal framework was tried in the patient’s mouth followed by ceramic build up and bisque try in. Final prosthesis was cemented using glass ionomer cement (Figure 6).
Post cementation instructions regarding periodontal maintenance were given. Recall was done periodically to assure the healing and success of the restoration

Figure 1: Intra oral view of cariously involved left mandibular 1st molar

Figure 2: Preoperative radiograph of cariously and periodontally involved lower left mandibular 1st molar

Figure 3: Radiographic view of lower leftt molar after endodontic treatment
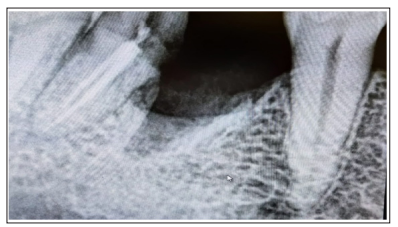
Figure 4: Radiographic view of lower left molar after hemisection of mesial port of root.

Figure 5: Tooth preparation done

Figure 6: Final prosthesis cemented
Loss of posterior teeth may result in several undesirable sequelae such as mesial drifting, loss of arch length, and loss of masticatory function. As previously discussed, treatment options for an extensively decayed and non-restorable molar are limited. A clinician must decide a treatment option based on the patient’s age, medical history, and the ability to maintain oral hygiene.1 In the present case, all possible treatment options were explained to the patient, including hemisection, as the decay was limited to distal root. Since the patient was young, she was reluctant to lose her tooth. In addition, her financial conditions made her to reject the option of dental implant. The long-term success of hemisected molar depends on a number of interrelated factors: periodontal condition of tooth, root anatomy, maintenance therapy, endodontic and restorative therapy, and the surgical procedure itself [3]. Buhler (1988) observed 32% failure rate in hemisection cases attributed to endodontic pathology and root fracture while other authors (0-9%) have shown a greater success in hemisection cases in the longterm studies [4]. The literature on distal root resection is limited as compared to mesial root in mandibular molars because of its anatomical structure [5, 6]. Nevertheless hemisection is a viable option to be considered before the extraction of molars specially in the presence of conditions such as severe vertical bone loss (one root of a multi-rooted tooth), furcation destruction, unfavorable proximity of roots of adjacent teeth, preventing adequate hygiene in maintenance of proximal areas and severe root exposure due to dehiscence [7]. Endodontic/restorative conditions which require hemisection are prosthetic failure of piers or abutments within a splint, endodontic failures, vertical fracture of one root, nonrestorable portion of a multi-rooted tooth [8]. In the present case, good prognosis was observed with proper occlusion, absence of mobility and healthy periodontal condition up to 6 months of follow-up. Concurring with previous reports, hemisection is a valid treatment option for the molar teeth’s in young children, which otherwise have to be extracted due to extensive caries. Thus, conservative management of extensive carious molar tooth along with periodontal involvement in young adult patients can not only preserve the tooth but also reduce the financial burden, psychological trauma and occlusal dysfunction [9].
Careful examination, proper diagnosis and sound knowledge along with the favourable prognosis can lead to the conservative management of cariously and periodontally involved molar which might have been extracted. Such conservative approaches not only save the dentition but also reduce the financial burden, psychological trauma, and occlusal dysfunction associated with tooth loss. Hemisection is an alternative, effective, and conservative treatment modality over conventional procedure or extraction of periodontally and endodontic affected teeth.