Author(s): Aicha Ibourk*, Ben Yahya and M. Bellamine
Odontoma is defined as a calcifying benign odontogenic tumor composed of various tooth tissues such as enamel, dentin, pulp, and cementum and representing the second most common odontogenic tumor of the jawbones. These lesions are often associated with impacted permanent teeth. They are usually small, asymptomatic and diagnosed after a routine radiographic examination.
The aim of this work was to report a case of a compound odontoma in the anterior maxilla of a 35-year-old woman, which was causing the impaction of the maxillary left central incisor. A removal of the tumor was planned. An orthodontic approach was proposed as a surgical procedure for orthodontic traction of the impacted tooth. After 12 months, the clinical and radiographic examination revealed the eruption of the impacted incisor.
The recommended treatment of compound odontoma is the complete removal of the tumor. An orthodontic approach may be indicated to correct any malocclusion or to perform the traction of the tooth, due to a possible impaction.
According to the 2017 World Health Organization classification, odontoma is an odontogenic benign tumor [1]. Odontoma is defined as calcifying benign odontogenic tumor composed of various tooth tissues such as enamel, dentin, pulp, and cementum and representing the second most common odontogenic tumor of the jaw bones [2].
They are typically divided into compound and complex odontomas although mixed forms have been described. Compound odontomas are formed by many little tooth-like structures often strictly adapted to each other and held together by a more or less complete connective capsule. They are easily recognizable; they are usually small but large lesions contain up to 100 denticles. Complex odontomas are formed by a single amorphous mass of mature odontogenic tissues without any structural organization, with tissues arranged in a more or less disorderly pattern [3,4].
These lesions are often associated with impacted permanent teeth. Impaction has been defined as the prevention of the eruption of a tooth to the expected times into a normal functional position due to the presence of an obstacle or reasons of different nature [5].
A 35-year-old woman was referred to the oral surgery unit with a symptom of swelling in the maxillary anterior sector associated with an unerupted maxillary left central incisor. The patient reported that she was a history of trauma at the age of 8. During the clinical examination, no facial asymmetry was detected extraorally. The clinical intraoral examination showed a swelling in the maxillary anterior vestibular sector, hard and painless on palpation and covered with a healthy mucosa and an unerupted maxillary left central incisor (Figure 1).

Figure 1: A swelling in the maxillary anterior vestibular sector, hard and painless on palpation and covered with a healthy mucosa, Unerupted central maxillary left incisor was noticed
Radiographic analysis revealed a radiopaque mass with multiple small structures, obstructing the eruption of the permanent incisor; the central maxillary left incisor situated in an included high position near the nasal fossae (figure 2 and 3).

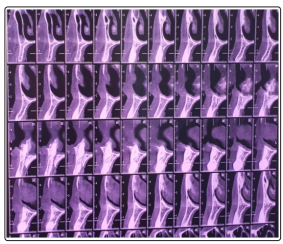
Figure 2 and 3: Presence of a radiopaque mass with multiple small structures, obstructing the eruption of the permanent incisor. - Central maxillary left incisor situated in an included high position near the nasal fossae.
On the basis of clinical and radiographic findings the provisional diagnosis of compound odontoma was made. The removal of the odontoma was planned. A mucoperiosteal flap on the labial surface of the lateral maxillary right incisor and left canine was reflected, with a surgical removal of the odontoma under local anaesthesia (figure 4 and 5).
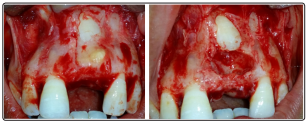
Figure 4 and 5:
- A mucoperiosteal flap on the labial surface of the lateral maxillary
right incisor and left canine was reflected
- Surgical removal of the odontoma under local anaesthesia
An orthodontic approach was proposed as a surgical procedure for orthodontic traction of the impacted tooth: collage of an orthodontic button in the labial surface of the central maxillary left incisor. The surgical flap was positioned and sutured in place (figure 6 and 7).

Figure 6 and 7: Collage of an orthodontic button in the labial surface of the central maxillary left incisor ans the surgical flap was positioned and sutured in place
After 12 months, the patient returned for a review appointment. The clinical and radiographic examination revealed the eruption of the impacted incisor (figure 8 and 9)
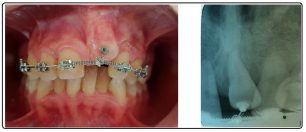
Figure 8 and 9: After 12 months: clinical and radiographic examination showed a progressive eruption of the central maxillary left incisor

Figure 10 and 11: After 24 months: clinical and radiographic examination showed a complete eruption of the central maxillary left incisor
Odontomas are nonaggressive, hamartomatous developmental malformations or lesions of odontogenic origin appearing as small, solitary, or multiple radiopaque lesions found on routine radiographic examinations. They are the most common odontogenic tumors which constitute 22% of all the odontogenic tumors of the jaws [6,7].
The etiology of odontomes remains unknown. It has been associated with various pathological conditions, like local trauma, inflammatory and/or infectious processes, mature ameloblasts, cell rests of serres (dental lamina remnants) or hereditary anomalies (Gardner’s syndrome and Hermann’s syndrome), odontoblastic hyperactivity, and alterations in the genetic component responsible for controlling dental development [8]. In this case, the etiology is a local trauma. Usually, compound odontoma is found more often in the anterior maxilla, whereas the rare complex odontoma usually develops in the mandible [9].
The incidence of compound odontome ranges between 9% and 37%. The majority of odontomas in the anterior segment of the jaws are compound composite in type (61%), whereas the majority of odontomas in the posterior segment are complex composite in type (34%). Interestingly, both types of odontomas occurred more frequently on the right side of the jaw than on the left, (compound 62% and complex 68%). The compound composite odontome most frequently occurred in incisor cuspid region of the upper jaw in contrast to the complex odontomeswhich were commonly found in molar and premolar region of the mandible [8]. In our case, compound odontome located in the anterior maxilla.
Both complex odontoma and compound odontoma were showed to cause disturbance in the tooth eruption as determines impaction or delayed eruption, associated with other conditions as malocclusions and temporomandibular joints disorders, displacement and of adjacent teeth, rganized ons, ankylosis, dentigerous cysts, and periodontal disease.
Most of the odontomas are asymptomatic and are discovered during routine radiographic investigations and can cause disturbances in the eruption of the teeth, infrabony defects and most commonly delayed eruption or deflection [9]. The case described an asymptomatic odontoma associated with an unerupted maxillary left central incisor.
Radiographic examination seems to be the most effective clinical method of differentiating between the two types. Compound odontoma, which radiographically shows comparatively a wellorganized malformed teeth or toothlike structures, usually is a radiolucent cyst like lesion whereas complex odontoma shows an irregularly shaped oval radiopacity usually surrounded by a well-defined thin radiolucent rim [8]. In our case, Radiographic analysis revealed a radiopaque mass with multiple small structures, obstructing the eruption of the permanent incisor.
Histologically odontomas consist of epithelial and mesenchymal tissues and their cells with apparently normal morphology. These tissues show a disordered arrangement in complex odontomas, whereas compound odontomas with miniature teeth-like structures show a well rganized tooth-like relationship of tissues. This indicates a higher degree of differentiation of cells in compound odontomas as compared with the complex odontomas [3,10].
Odontomas are treated by traditional surgical elimination, and there is small likelihood of recurrence. The extent of damage to the teeth enhances with a later diagnosis and early detection, and removal of odontomas seems to be associated with a better prognosis for the impacted teeth. The prognosis of spontaneous tooth eruption after odontoma removal has been reported to be predictable; however, the orthodontic- surgical approach was showed to be warranted for correct tooth positioning. Evaluation of the extent of root development by radiographic examination during periodic observation is also useful for establishing adequate occlusion after surgery. Incomplete closure of the root apex of the impacted permanent tooth at the beginning of orthodontic therapy might have contributed to the favorable results. Although permanent teeth are sometimes extracted in association with the removal of odontomas [9].
Treatment options also include simple observation with periodic clinical and radiological checkup, to evaluate the development of these teeth. A number of different techniques have been proposed for osteotomy: ultrasonic, CO2, high-speed rotary handpiece, piezosurgery, and the erbium laser. The laser technique has a number of advantages, including precision, conservative action with less bone destruction, lack of vibrations, decontamination, and reduction of postoperative edema. However, there are also some disadvantages, including lengthening the time required for surgery, and the fragility of the surgical tips, which can easily break leading to higher costs [11].
In our patient, a clinical and radiological checkup was done every 6 months. After 24 months, a complete eruption of the impacted teeth was made.
The orthodontic alignment of an impacted tooth to its normal functioning position in the oral cavity may require prolonged and complicated treatment. Prognosis and treatment difficulty can be affected by many factors, some of which are related to the patient, others to features associated [12].
In our case, a removal of the odontoma was planned followed by an orthodontic alignment of an impacted tooth.