Author(s): Diani A*, Azzahiri I, Benfaddoul O, Zouita B, Basraoui D and Jalal H
Osteomas are a type of benign tumors that can develop in various bones of the skull. The fronto-ethmoidal region is the most commonly affected site, with over 50% of cases being reported in this location. The temporal bone, particularly the mastoid and external auditory canal regions, is another frequent site of osteoma formation. However, the occurrence of osteomas within the middle ear is relatively uncommon. The presence of osteomas within the internal auditory canal is a rare phenomenon and has been reported infrequently in the medical literature.
Cranial osteomas are benign tumors that can develop in different bony parts of the skull, The fronto-ethmoidal location is the most common. The fronto-ethmoidal location is the most frequent in more than half of the cases [1-3]. The temporal bone can also give rise to these tumors especially in the mastoid, external auditory canal and more rarely the middle ear, the localization in the internal auditory canal is very rare, only a few cases have been described in the literature [4-6].
Internal auditory canal osteoma is often asymptomatic and is discovered incidentally during a facial or brain CT scan for another indication, showing a well-circumscribed, sometimes poly-lobed, pedunculated lesion of bone density [7].
The modalities of choice for visualization of internal auditory canal osteomas are CT with with thin sections (CT of the rock) and magnetic resonance imaging (MRI).
Magnetic resonance imaging (MRI) with dedicated sequences for the rock [1]. In absence of neurosensory symptoms and surgical indications, the diagnosis can be made on the diagnosis can be made on the basis of radiological characteristics alone.
We present the case of a 17-year-old girl presenting with left otological symptoms left otologic symptomatology and in whom a CT scan of the rock discovered incidentally an osteoma of the right IAC.
A 17-year-old girl, without any particular pathological history, presented with hypoacusis and left tinnitus evolving for two months. Otoscopic examination found a left retraction pocket grade I of the lower half of the tympanic membrane and a perfectly normal right eardrum. The audiogram showed a mixed hearing loss on the left and no abnormality on the right.
The patient was referred to us for a CT scan of the two rocks, which showed no abnormality on the left, in particular no mass syndrome or filling of the middle ear (figure 1). The analysis of the right rock showed the presence of a bony growth on the anterior wall of the internal auditory canal porus, pedunculated, with regular contours, the diagnosis of an osteoma of the IAC was retained (figure 2). We conducted a supplementary brain MRI utilizing T2 FSE coronal HR, T1 millimetric, and FIESTA sequences to examine the cerebellopontine angle. The objective of the MRI was to identify the formation of lesions, which was achieved by analyzing T1 isosignal, T2 hyposignal, and FIESTA images. Upon analysis, there was no evidence of acoustic-facial bundle involvement.” (Figure 3).
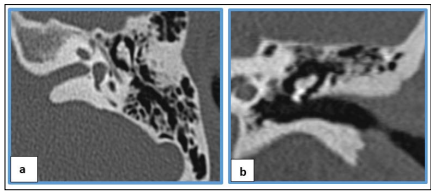
Figure 1 : Normal CT scan of the left rock in axial (a) and coronal (b) sections
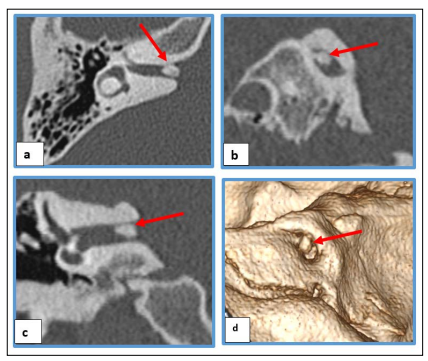
Figure 2: CT scan of the right rock with multiplanar reconstruction in axial(a), sagittal(b) and coronal(c) and 3D(d) sections showing the osteoma of the IAC at the expense of the anterior wall of its porus(arrow).
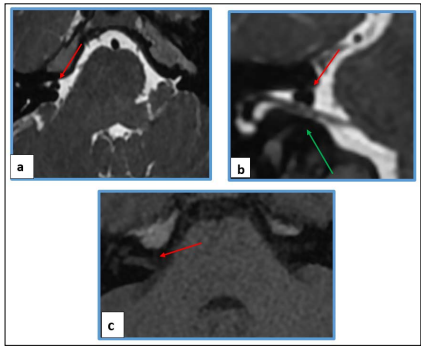
Figure 3: MRI of the cerebellopontine angle in high resolution T2 sequence (FIESTA) with axial(a) and coronal(b) reconstruction and in T1 sequence millimetric cuts(2mm) showing the osteoma of the right CAI porus in frank T2 FIESTA hyposignal and T1 isosignal (red arrows) and its intimate contact with the acousticfacial bundle (green arrow).
The diagnosis of osteoma of the internal auditory canal was retained. The patient was asymptomatic, and monitoring of the patient was recommended.
Internal auditory canal osteoma is a very rare entity, only a few cases have been described in the literature. The most common locations of osteomas reported in the literature are the external acoustic meatus and mastoid, the facial bones and the mandible. Several factors have been proposed as causes of internal auditory canal osteoma including repeated trauma, infection, inflammation, hormonal factors and constant vascular irritation [6-9].
The clinical presentation is variable, it can be asymptomatic of fortuitous discovery during a radiological examination (incidentaloma), the clinical symptomatology is related to the narrowing of the canal and the compression of the acousticofacial bundle and manifests itself by vestibular signs with vertigo and balance disorders and auditory signs with progressive loss of hearing and tinnitus. The facial nerve is usually spared until very late in the course; the greater resistance of the motor facial nerve to compression in CAI is fairly well recognized. A review of the literature by Suzuki et al (2014) of 17 cases of CAI osteoma identified several clinical features, namely: a mean patient age of 44.1 years (male:44; female:44.2), a female-to-male sex ratio of 1.4:1, bilateral localization for 2 cases. Six cases were identified incidentally (12%), including our case who was asymptomatic on the affected side at detection, 7 cases had subjective or objective hearing loss (41%), 10 cases had tinnitus and/or auditory fullness on the affected side (59%), 11 cases had vertigo and/or dizziness (including medical history) (65%), and 2 cases had facial palsy [6-12].
Biopsy for histological study can confirm the diagnosis of osteoma by demonstrating fibrovascular ducts surrounded by lamellar bone with few osteocytes, but it is dangerous given the location of the internal acoustic meatus [7, 16, 18].
The treatment of this pathology remains controversial. Osteomas are slow-growing tumors, remain asymptomatic for a long time, and should be followed up by clinical and imaging. In patients with cochleovestibular symptoms, a trial of symptom-targeted therapy should be performed, and surgery should be considered only if the patient does not improve. In fact, the role of surgery remains to be determined, and the exact indications for surgery remain to be defined [1, 7].
The location of osteoma in the internal auditory canal is exceptional. Its appearance is similar to that of other bony locations. The seriousness lies in the risk of compression with a suffering of the acoustico-facial bundle.