Author(s): Renata Indelicato Zac*, Luiz Fernando de Oliveira Santana and Adilson da Costa
Granuloma annulare (GA) is a common, benign, chronic inflammatory disorder, which is characterized by grouped papules in an annular shape. It has been described in several clinical subtypes, including localized, generalized, subcutaneous, perforating, and erythematous. Herein, we report a 65-year-old woman with pruritic erythematous patches, mimicking mycosis fungoides, which occurred on the abdomen and thights and showed typical clinical and histopatologic findings of erythematous GA.
A 65-year-old white woman was referred to our clinic with a 2-year history of asymptomatic erythematous patches increasing in diameter on her abdomen and thighs.
Examination of the abdomen and thighs revealed large erythematous, non-scaly, oval patches, with no induration or atrophy (Figures 1 & 2). Skin sensitivity tests were normal. Physical examination was otherwise unremarkable.
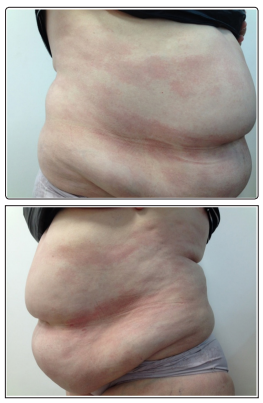
Figure 1 & 2: Erythematous oval patches, non-scaly, with no induration or atrophy on the abdomen
Histopathological examination revealed a moderate superficial and mid-dermal interstitial infiltrate of lymphocytes and histiocytes, and mucin between collagen fibers (Figure 3). These findings are consistent with the interstitial variant of granuloma annulare [1].
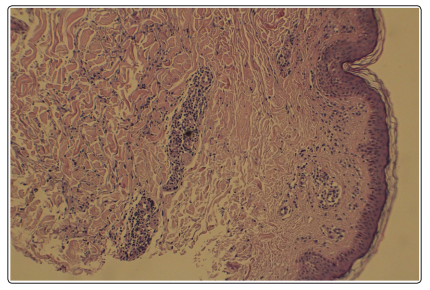
Figure 3: Moderate superficial and mid-dermal interstitial infiltrate of lymphocytes and histiocytes, and mucin between collagen fibers
The diagnosis of patch-type granuloma annulare was made, and the patient was treated with tacrolimus ointment twice daily for 8 weeks with no improvement. Then, tacrolimus was withdraw and hydroxychloroquine was started at a dose of 200mg/day. After 8 weeks, lesions on the abdomen partially improved, while lesions on the thighs disappeared completely (Table).
Granuloma annulare (GA) is an idiopathic benign, granulomatous skin disease characterized by skin-coloured or erythematous annular dermal papules and plaques with female predominance [2]. The condition is generally asymptomatic, although there may be some pruritus or even pain [2].
Flat patches of granuloma annulare are rare and may be challenging to distinguish between other conditions, such as mycosis fungoides, interstitial drug reaction, erythema anulare centrifugal, reticular erythema mucinosis, and lupus erythematosus profundus [3].
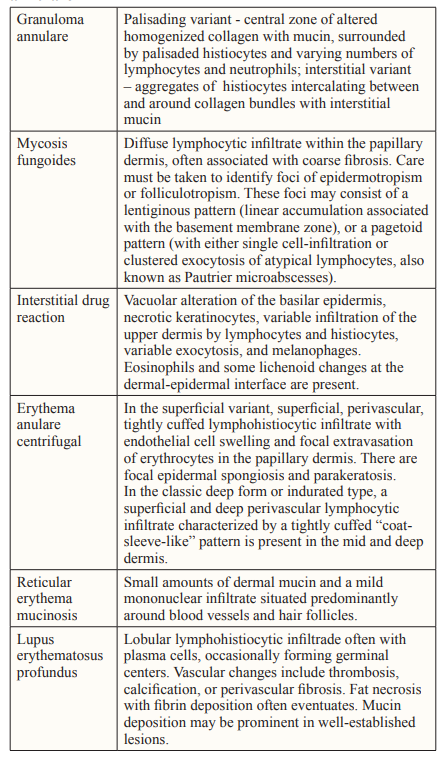
Source: Elder DE. Lever’s Histopathology of the Skin. Philadelphia: Lippincott Williams and Wilkins, 2005
It is reported that patch granuloma annulare will respond to the same therapy as other types of granuloma annulare [2]. The size and localization of granulomatous lesions and the related diseases definitely influence the choice of treatment [2].
In several case reports, topical tacrolimus and pimecrolimus showed positive outcomes [2]. The exact mechanism of action of pimecrolimus and tacrolimus in GA is not clearly established [2]. The incidence of side-effects is low [2].
When available and acceptable to the patient due to time requirements, phototherapy may be tried [2]. Long-term use may lead to actinic damage localized to treatment areas and an increased risk of cutaneous malignancy [2].
If treatment with topical corticosteroids or phototherapy is impractical or ineffective, we suggest systemic treatment with hydroxychloroquine, isotretinoin or dapsone as first choice. Fumaric Acid Esters are mentioned as a second-line treatment option in GGA [2]. Adverse effects include usually mild flushing and gastrointestinal symptoms [2]. Relative lymphopenia is the most frequent laboratory finding in long-term treatment [2]. Resolution of patch-type granuloma annulare after biopsy has been reported [4].
Long-term maintenance therapy has been necessary for prolonged clearance of disease [2]. The described systemic therapies are all immunosuppressive with potential side-effects [2]. Effective therapies with minimal side effects are needed [2].
In conclusion, we present a rare variant of granuloma annulare characterized by patches of erythema on the trunk and thights that mimick micosis fungoides but display the classic histopathological findings of interstitial granuloma annulare and that showed good response to hydroxychloroquine.