Author(s): Javier Castaneda-Lopez MD, Julissa Castro PT, Liliana Medina PT, Manuel Alfonso Banos- González MD, Cuauhtemoc Vasquez-Jimenez MD, Víctor Hugo Varela Cervantes MD and Alex Augusto Flores-Galaviz MD
The incidence of cardiovascular events and the rehabilitation of afflicted people are ways to reduce cardiovascular diseases, which is why cardiac rehabilitation
programmes are crucial. Cardiovascular diseases are the leading cause of death worldwide. Anaerobic training, which we can develop our muscular strength
through various methods, is a significant sort of exercise in these programmes. The purpose of our study is to show that resistance band strength training
is safe for individuals undergoing cardiac rehabilitation.
Ischemic heart disease, which affects more men than women (58% vs. 42%), is the most common form of cardiovascular disease and the leading cause of mortality globally. The WHO also advises people who have experienced a cardiovascular event to enrol in a cardiac rehabilitation programme since they can improve their quality of life and lower their risk of future cardiovascular events. It has been demonstrated that, when combined with adequate medical care, it lowers the number of cardiovascular fatalities, cardiovascular event recurrences, and hospitalisations while also enhancing quality of life and having a favourable cost- effectiveness profile [1-3].
The Cardiac Rehabilitation Programme (CRP), as described by the WHO in the 1960s, is "the set of measures necessary to ensure optimal physical, mental, and social conditions for heart patients that allow them to occupy as normal a place as they are able in society [1]."
Anaerobic exercise, which is one of the CRP's components, aims to increase physical attributes like strength, joint mobility, flexibility, coordination, and balance [4]. Although muscular strength is a crucial physical trait for the development of fundamental human activities, it has received little attention in the population at risk for cardiovascular disease because there are no precise terms for the physiological effects attained, which have long been the subject of debate and divergent opinions among researchers [5].
According to some studies, resistance training lowers cardiovascular risk. Some of the biological factors that contribute to this relationship include increased muscle mass and decreased visceral fat, which leads to better glucose regulation, metabolic dysfunction, and inflammation. Other physiological effects of these workouts include better blood flow throughout the body, increased oxygen delivery to muscles, and improved coordination, balance, and muscle flexibility [6].
Despite continuing the trend of using elastic bands to increase muscular strength, significant effects on flexibility and other physical qualities, including posture, gross and fine motor skills, proprioception, gait, quality of life, and pain, have been discovered [5].
It had been thought that the rise in arterial stiffness, which led to left ventricle hypertrophy as a result, was one of the drawbacks of resistance training in those with heart disease [6]. However, it has been demonstrated that strength training at intensities of 40-50% of maximal contraction does not result in disproportionate increases of the double product, achieving a reduction in myocardial oxygen consumption, with the ensuing reduction in ischemia and improvement in angina symptoms [4].
Resistance training has additional advantages for people with
ischemic heart disease, including:
• Enhanced muscle endurance and strength.
• Lessened heart workload during routine activities.
• Increased functionality and performance on a daily basis.
• Osteoporosis, diabetes, and obesity prevention and therapy
in addition to these conditions.
• An increase in independence and self-confidence on the
physical front.
• Lessening of the ageing-related loss of muscular mass and
strength [7].
With regard to the negative consequences, it is challenging to properly ascribe causation for or against it because there aren't many research that have just employed elastic bands for strength training. There aren't enough studies of this kind of training in particular pathologies that support the use of elastic bands in such situations, despite some research showing significant differences in favour of the interventions using elastic bands [5]. This study's goal is to show that using resistance bands for strength training in heart patients enrolled in cardiac rehabilitation programmes is safe.
The safety and outcomes of resistance band strength training in patients with heart disease participating in phase II of the Cardiac Rehabilitation programme were the subject of a descriptive and retrospective investigation.
Patients who completed phase II were included, who complied with all the training sessions, who did not have any limitation or contraindication to perform strength exercises with resistance bands, those patients who had some limitation or in whom we did not have the necessary data from the initial and final evaluation according to the Lovett scale were excluded.
At the start and completion of treatment, all patients had an objective, analytical, and functional evaluation of their physical characteristics using goniometry, the Lovett scale, the Seat and Reach test, the Elly, and the Thomas test.
The strength training programme was carried out while the heart and blood pressure were being continuously monitored. The heart rate was recorded, the blood pressure was checked before and after the workout, the effort level was graded using the Borg scale, and arrhythmias that developed were noted. The strength training programme was created on an individual basis while adhering to safety guidelines and the training prescription. Within the parameters of the target HR and double target product, progression was made in accordance with perceived exertion.
Resistance bands of different resistance and tension were used, the routines were 3 sets and 10 repetitions, working lower and upper limb muscles, both agonists and antagonists. Usually, the progression began from the third session until the maximum tolerance to the resistance and tension of the league.
For quantitative variables, means and standard deviation were used in descriptive statistics, and for category variables, absolute values and percentages were used Categorical variables were compared using the chi square test, and related samples were compared using the T test. A p value of 0.05 or less was regarded as significant. The statistical software SPSS version 22 was employed.
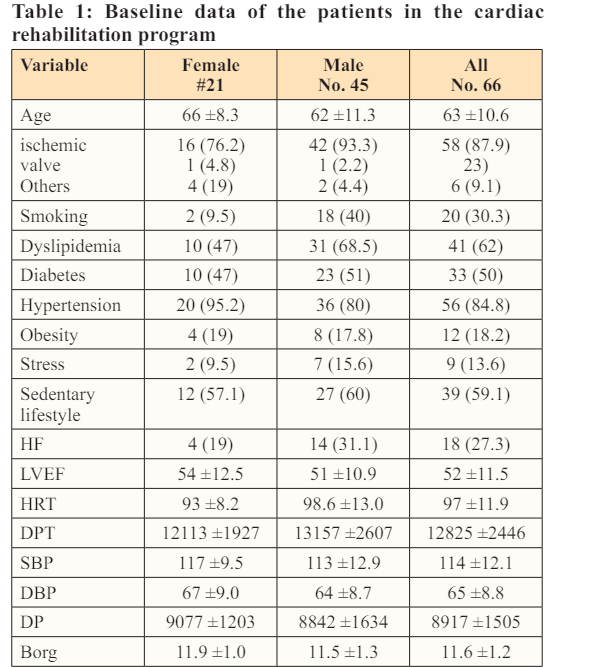
Sixty six patients in total, 45 men and 21 women, with average ages of 62 and 66, respectively, were included. Ischemic heart disease was the most common diagnosis, and the majority of the patients had systemic arterial hypertension, dyslipidemia, and were sedentary
The majority of patients had ischemic heart disease, dyslipidemia, and systemic arterial hypertension. Of the total patients, 18 had heart failure with a low ejection fraction, and the remainder of the demographic data is provided in Table 1.
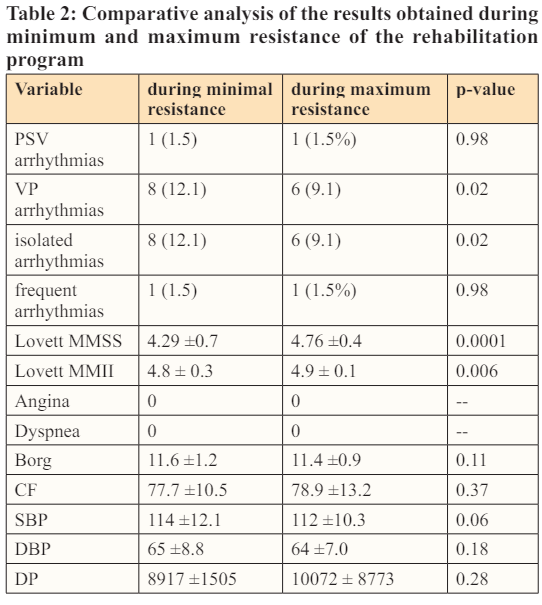
During the training we observed that all the patients tolerated according to the perception of the intensity of the effort with the Borg scale, which was slightly higher in the session where minimal resistance was applied, no patient manifested angina or dyspnea during the resistance exercise. Some patients presented isolated ventricular extrasystoles mainly in the first sessions (minimum resistance) which decreased in the last sessions (maximum resistance). This being statistically significant, only one patient presented frequent ventricular extrasystoles in both sessions, systemic blood pressure was lower in the maximum resistance session, although the heart rate was slightly higher in the maximum resistance session, therefore, we observed that the double product was greater in the maximum resistance session, which may suggest an increase in oxygen consumption, it is possible to It should be mentioned that this fact did not trigger signs or symptoms of ischemia or the presence of arrhythmias, in the rest of the hemodynamic parameters measured both in the minimum and maximum resistance sessions (HR and SBP) there were no statistically significant differences.
The patients who participated in the cardiac rehabilitation programme said they felt physically better after completing it. They feel more secure performing their regular duties as a result of the development in muscle power, particularly in the lower limbs.
Regarding the improvements in muscle strength, we saw that there was a statistically significant improvement between the final and initial Lovett Assessments for both the upper and lower limbs; Table 2.
Our results showed a slight decrease in systolic blood pressure with a slight increase in heart rate, this without clinical or electrocardiographic evidence of ischemia and/or arrhythmias. Hernandez et al. demonstrated that resistance exercises had the effect of increasing systolic blood pressure without increases in heart rate [8].
Maroto showed that low-intensity training, defined as contractions between 40 and 50 percent of maximum, does not result in disproportionate increases of the double product, resulting in considerable reductions in myocardial oxygen consumption, as well as a reduction in ischemia and angina symptoms [3]. However, in our investigation, we discovered that the maximum resistance session experienced a double product increase without the patients exhibiting any signs of ischemia [5].
According to a meta-analysis, strengthening exercises for patients with coronary heart disease improved their muscle strength without causing any complications. We observed a similar pattern with our findings because, as measured by the Lovett scale, our patients' upper and lower limb strength increased without any signs of cardiovascular complications [3].
Similar to the study conducted by Madaria, our patients engaged in strength training with elastic bands, gradually increasing the resistance until they reached the maximum acceptable resistance. As a result, we saw an improvement in the programme's assessment of muscle strength. rehabilitating as well as raising one's standard of living [7].
Resistance exercise overload should be avoided because it can raise blood pressure, which can lead to ischemia due to a double product increase, heart failure due to an increase in left ventricular end-diastolic pressure, and arrhythmias due to sympathetic hyperactivity-even if heart rate does not change significantly. Due to the lack of complications or cardiovascular events during the cardiac rehabilitation program, our training protocol was therefore restricted to the hemodynamic parameters prescribed at the beginning of the programme and the perception of effort according to the Borg scale.
As previous studies have shown, resistance exercise overload can lead to increased blood pressure and should be avoided, and even in the absence of significant changes in heart rate, an increase in the two-fold product can It may lead to blood data. Heart failure due to elevated left ventricular end-diastolic pressure and arrhythmia due to sympathetic hyperactivity [4]. For this reason, our training protocol was limited to exercise perceived according to the Borg scale and hemodynamic parameters prescribed at program initiation, with no evidence of complications or cardiovascular events during the program of cardiac rehabilitation.
Based on our results, strength training in cardiology patients is safe as long as it works within safe parameters, monitors heart rate and blood pressure, and measures effort according to the Borg Scale. It is important that the patient avoid performing the Valsalva maneuver during strength training to avoid any alteration such as an increase in intra-abdominal and intrathoracic pressure.
The diagnosis, type of procedure, time of evolution and tolerance to effort should be considered for planning the exercise routine. Although our population is small, we believe that, like other studies, strength training with resistance bands in patients in cardiac rehabilitation programs is safe and useful, if the recommendations and limits of hemodynamic parameters are followed prescribed [9-22].