Author(s): Lashkar Pravalika*, Heena Fathima, Sirikonda Jyotsna and T Ravi Chander
Each year many patients are hospitalized due to adverse drug reactions. Amoxicillin is a broad spectrum , bactericidal, beta lactum antibiotic, commonly used to combat various infections. Pencillin group of drugs are known to cause cutaneous drug eruption especially in pediatric population. Paracetamol is used as antipyretic and analgesic Steven Johnson syndrome is an acute, self limited disease, presenting as severe mucosal erosions with wide spread erythematous, cutaneous macules. Majority of cases are drug induced affecting oral and peri- oral region. Aim of the article is to present a case of steven Johnson syndrome primary to drug therapy amoxicillin and paracetamol. A 14 years female patient was admitted in hospital with a chief complaints of blisters over tongue, lips, difficult in swallowing, patient was dehydrated and fever since 5days. The reaction was evoked after consumption of tab amoxicillin, and paracetamol. She was treated with corticosteroids, local anesthetic, antiseptic, antifungal, iv fluids. Health care provider must be carefully regarding the adverse effect of drug especially Steven Johnson syndrome which is a potentially fatal condition. The case being reported to emphasize the need for pharmacovigillance in order to motivate adverse drug reaction reporting so as to gather more data regarding adverse drug reaction.
Cutaneous eruption is one of common forms of adverse reaction manifestation. Adverse drug reactions (ADRs) hold special importance in healthcare as they account for 6% of total hospital admissions, increase in economic burden on healthcare system, withdrawal of drugs from market, and death [1]. SJS is one such manifestation. Stevens-Johnson syndrome (SJS) is a rare, serious disorder of the skin and mucous membranes. It’s usually a reaction to medication that starts with flu-like symptoms, followed by a painful rash that spreads and blisters. Then the top layer of affected skin dies, sheds and begins to heal after several days [2]. Steven-Johnson syndrome (SJS) is an infrequent and a severe form of erythema multiforme (EM). It can occur due to an adverse hypersensitivity reaction to drugs which results in skin and mucosal eruptions that can be potentially fatal. It is considered to be a less severe form of toxic epidermal necrolysis (TEN) [3]. The basic difference between SJS and TEN is the percentage of body surface area (BSA) involved: <10% in SJS; >30% in TEN; 10 to 30% in SJS-TEN overlap [4].It is caused by a hypersensitivity reaction, usually to drugs (e.g. - salicylates, sulfonamides, penicillin, barbiturates, carbamazepine, phenytoin) but it is also seen with infection or cancer. There is ulceration of skin and mucosal surfaces. Typical target lesions develop, often on palms or soles with blistering in the centre [5].
SJS may present as a nonspecific febrile illness (malaise, fever, vomiting, headache, cough, rhinorrhea) with polymorphic lesion on skin and mucous membrane characterized by blisters and erosions [6]. Drugs are most commonly implicated for causing 77-95% of cases [7]. The incidence of SJS has been estimated to be around 1-6/1,000,000 persons per year with a mortality rate of 1-5% which rises up to 30% in TEN. Multiple drugs have been identified to cause SJS and TEN, antibiotics (sulfonamides) being the most common [8]. Diagnosis is based on the appearance of skin lesion and a history of risk factors or related disease [9]. The exact mechanism of SJS still remain unknown. It has been well established that the epidermal damage in these diseases is due to keratinocyte apoptosis. Although drug-specific T cells are implicated in this process, our understanding of the immunopathology is far from complete [10]. SJS/TEN reactions are believed to follow type IV hypersensitivity reaction in which a drug or metabolite stimulates cytotoxic T cell (i.e.CD8+ T cells) and T helper cells (i.e. CD4+ T cells) to initiate auto immune reaction that attack self tissues [11].
A 14 years old female patient living in hostel presented with history of fever and sore throat to a local doctor for which she was prescribed with capsule amoxicillin 250 mg bidx 5 days and tablet paracetamol 500mg tidx5 days, tablet ranitidine xod 5 days.
After consumption of first doses of medication, she didn’t experience any sign/symptoms after taking the 3 dose patient developed blisters over lips and tongue. She again visited the doctor and prescribed with chlorpheniramine maleate 4 mg bid x 3days, cetirizine 5mg bid x 3days.. and symptoms are worsened into difficult in swallowing and drinking water and she became dehydrated. After 2 days she presented to Mahatma Gandhi Memorial Hospital.
•General examination
• On examination patient was conscious and coherent , a febrile,
blood pressure -90/60 mmHg, pulse rate - 92 b/min.
• Local examination
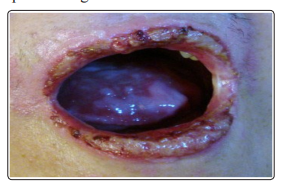
Ulcer over lips and tongue.
All the routine investigations were performed and revealed RBS - 53mg/dl, SGOT- 32U/L, SGPT- 14U/L.
Both amoxicillin and chlorpheniramine maleate were withdrawn immediately.Patient was treated immediately with IV fluids 1 pint normal saline for dehydration.
Multiple therapies were prescribed to the patients. Ointment betamethasone dipropionate 0.05% bid, benzocaine 1% bid, zinc oxide 2oz bid, povidone iodine 2% gargle bid, benzocaine syrup 5ml bid, clotrimazole 1% oral bid for ulcers prescribed for 6 days. on 3rd day patient complaining of throat pain she was prescribed with tab mefenamic acid 500mg bid x4 days. Blisters are healing. On 5th day patient complaining of cough and prescribed with ambroxyl syrup 5ml bidx 3 days. No fresh complaints .Patient recovered from this fatal adverse reaction after rigorous treatment for 10 days .She was discharged with advice to continue topical antibiotics for oral blisters .On follow up visit, after a week the oral blisters had completely healed.
Adverse drug reactions (ADRs) hold special importance in healthcare as they account for 6% of total hospital admissions, increase in economic burden on healthcare system, withdrawal of drugs from market, and death [12]. The cutaneous drug reaction are among the most commonly reported adverse reaction.SJS is considered as rare severe skin condition affects mucous and skin membrane. The extent of total skin surface involvement is less than 10% .SJS mostly happen in first 2nd month of intake of drug, severe in 3rd month .It is mainly start with fever ,flu ,blisters on skin, mucous, nose and genitals later painful red or purple skin, watery eyes appear. Cytotoxic T lymphocytes play a major role in pathogenesis. In clinical practice, these reactions are manifestation of drug -induced hypersensitivity. The etiological factors of SJS can be range from viral infections to various pharmacological agents [13]. As stated earlier, penicillin group of antimicrobial are common antimicrobial agents cause cutaneous drug eruptions.
Scientists are not certain why SJS develops. The most commonly cited cause of SJS is an adverse allergic drug reaction .Till date few cases of amoxicillin induced SJS have been reported. Currently no treatment modality has been established as standard for these patients. The combination of drugs like amoxicillin - clavulanic acid and dicloxacillin causing SJS were prescribe and examine carefully [14] . However the paracetamol is the safest drug taken in combination with amoxicillin but few cases are reported that paracetamol can also cause cutaneous adverse drug reaction (SJS) so, before prescribing the drug , dosage adjustment and duration should be done properly [15]. Early diagnosis with prompt recognition and with drawl of all potential causative drug is essential for favorable outcome [2].
Beta - lactam group of antimicrobial are promptly associated with severe cutaneous adverse drug reaction (CADRS) like SJS. Although these CADRS are predominantly mild in nature, they can be severe in manifestation at any time. Scientists are not certain why SJS develops. The most commonly cited cause of SJS is an adverse allergic drug reaction .SJS occurs twice as often in men as women, and most cases appear in children In developing countries like India ,where the infectious disease are widely prevalent ,the frequent use of beta - lactam antimicrobial and subsequent ADRs cannot be avoided. Reporting of such event is utmost necessary, efficient in pharmacovigilance holds key in this regard.
The authors declare no conflict of interests.