Author(s): Mahfouth Ahmed Almansory*, Mohamed Ahmed Qazit and Ahmed Ali Khalaf
Background: Vegetables and fruits are an important part of a healthy diet and help with growth and support body functions and physical, mental, and social well-being at all ages. They can also help prevent all forms of malnutrition, such as undernutrition, micronutrient deficiencies, obesity, and overweight, and reduce the risk of non-communicable diseases. World Health Organization consumption of at least 400 grams of fruits and vegetables per day, or five servings of 80 grams each, and the reasons for the sad fact that most people do not eat enough of them to maintain a healthy life for the sake of obesity treatment and weight reduction.
Objectives: The aim of the study was to investigate the effects of increasing fruit and vegetable intake rich in antioxidants and vitamins on people at risk of obesity and high levels of blood fat and to provide education about its benefits and the amount of daily rations.
Methods: This a descriptive cross-sectional study, 160 obese women underwent to Aspetar ospital in Misurata city during The period (October–December 2022) and they were divided into two groups of 80 women per group. The first group was presented with a weight-loss diet devoid of vegetables and fruits. The second group was given a weight-loss diet rich in vegetables, including cucumber, lettuce, tomato, and fruits (kiwi, apple, and orange). For three consecutive months.
Results: The findings were a decrease in weight with an average of 8 kg per woman for the first group and 15 kg per woman for the second group, and the average cholesterol and triglycerides were 280 mg/100 dL of blood and 230 mg/100 dL of blood, respectively, for the women of the first group. While it was 150 mg/100 dL blood and 90 mg/100 dL blood for the women of the second group, with some daily light exercise for all women in the two groups. Conclusion: This study indicates that consumption of three to five portions/day of fruit and vegetables is highly associated with prevention and a low risk of obesity, high blood fat, cholesterol, and cardiovascular disease. Therefore, we recommend relying on eating vegetables and fruits daily to reduce weight and blood fats, improve health, and nourish the body.
Low consumption of plant-based foods, including fruit and vegetables, is associated with an increased risk of many Chronic non-communicable diseases affecting human beings. Including high blood pressure, cardiovascular disease, stroke, diabetes, and obesity. Libya ranks fifth in the Arab world in the prevalence of obesity among women. (Kuwait 55%, Egypt 48%, UAE 24.9%,
Bahrain 24.9%, Kuwait 55%, and Libya 24.9%). Women are considered obese in excess of 35 kg/m2 according to the BMI. The causes of obesity are inheritance, thyroid laziness, an unhealthy lungial regimen, taking cortisone tablets, or a lack of exercise. Its main complications include Type II diabetes, hypertension, arthritis, high triglycerides, and high blood cholesterol. To treat them, you must follow the regiment diet, exercise, and dissolve the subcutaneous grease through lipolysis and Lipid freezing [1-3]. For weight loss, therapeutic nutritionists recommend a diet rich in vegetables such as lettuce and tomatoes and eating specific portions of fruits. Such as apples, kiwis, oranges, and others rich in dietary fibers, antioxidants, vitamins, and minerals; most countries have food recommendations including fruits and vegetables; and the WHO recommends consumption of less than 400g of fruits and vegetables per day or five portions of 80g each useful in burning grease and reducing appetite for food [4,5].
In Western Europe and North America, high-income people consume only half the ideal quantities, while those in North Africa and the Middle East consume more despite the decline in income in these areas in general, and the diet lasts for 3 consecutive months at the rate of 3 meals/day by adding a snack meal, leading to low weight and blood fat [6-8].
The benefit lies in the cortex, so most public health doctors never like peeling fruit before eating. Legumes, especially beans, chickpeas, and lentils, are rich in fiber and can be eaten raw or cooked; oat bread or brown bread is one of the finest breads that can be eaten for those with digestive problems; it is also the basic meal in slimming programs; sweet corn, broccoli, peas, beans, cooked potatoes, oranges, and strawberries; and in order to keep us healthy for a longer life, we must search all the time for these foods that will provide us with natural fiber [9-13]. and food fibers abound in plant-based foods. Polysaccharides are non-digestible sugars in humans in the absence of enzymes. But it has other benefits. It helps fight constipation, promotes satiety, and is a source of kneading and water-soluble vitamins [14-17]. Dietary fibers are chemically composed of non-starchy carbohydrates such as cellulose, dextrin, inulin, lignin, wax, pectin, low-plurality sugars, legumes, oats, rye, and fruit barley [18-21].
Some vegetables, such as cauliflower, carrots, Jerusalem artichokes, root tubers, and root vegetables such as potatoes, onions, psyllium, linen, nut seeds, and almonds [21-23]. Biodegradable fibers absorb water and become gels during digestion; the process of digestion becomes slow, and food absorption from the stomach and intestines decreases. These fibers are found in oats, barley, nuts, seeds, beans, lentils, peas, and some fruits and vegetables [24-26].
Non-biodegradable fibers are found in wheat bran, vegetables, and whole grains (not removed from them). Apparently, it increases the speed of food passing from the stomach and intestines and increases the size of the stool. The average person these days eats 10–15 g/day of fiber, and experts advise children, adolescents, and adults to take 20–35 g/day. Young kids can’t eat too much to make it happen, so they recommend eating cereals, fresh fruits, and other foods rich in fiber. To secure an adequate intake of fiber, you have to eat a variety of foods, including more fruits, whole grains, vegetables, beans, and peas, and increase your fiber intake gradually over a few weeks to avoid abdominal pain [13,25,27].
Water helps fiber pass through the digestive tract. Drink a lot of fluids (about eight cups of water or calorie-free liquids every day). Peeling (removing the crust from fruits and vegetables) reduces the amount of fiber in food; cooking may actually increase the amount of food eaten because it decreases the amount of food prepared. Therefore, eating foods containing fiber is useful, whether cooked or raw. The American Foundation of Medicine recommends that a person take dietary fibers daily according to the following table: The daily need for dietary fiber is about 30–50 g/for males and 20–30 g/day for females. Half a cup of fruit contains approximately 2 g of fiber, and half a glass of vegetables contains 2–3 g. For legumes, half of the cup contains 6–8 g of fiber [27,28]. Overweight or obesity is a contributing factor to an increased risk of high fat and cholesterol levels in the blood and leads to the risk of many diseases and health problems, such as hypertension and heart disease. The aim of the study was to investigate the effects of increasing fruit and vegetable intake rich in antioxidants and vitamins on people at risk of obesity and high levels of blood fat and to provide education about its benefits and the amount of daily rations.
Data collection: Data collected for a randomized clinical trial of follow-up cases of 160 obese women with BMI > 35 kg/m They were 15–50 years old, and their weight (kg), waist circumference (cm), and buttock circumference (cm) were measured. Blood triglyceride levels and blood cholesterol levels (mg/dl) were tested. From various Libyan cities among the frequents of the therapeutic nutrition clinic at Aspitar Hospital in Misrata city during the period (October–December 2022).
Diet Regimen: Designed 2 diets for this research: Diet 1 (1800 KB Price/day) and diet 2 (2200 KB price/day). Spread over 3 meals (breakfast, food, and dinner) separated by 6 hours (8-2-8). Few starches and desserts rich in meat, vegetables, and fruits for 3 months (October–November–December 2022), all cases also underwent 5-7 fat fragmentation sessions (Fat splitting) using a Turkish-made Cryolipolysis device that emits different frequencies of ultrasound. Fat-freezing physical and vital measurements were re-measured and the data monitored.
Out of 160 obese women taken up for the study, The age ranged from 15 to 50 years. The age of the participants was divided into seven age groups: 15–19, 20–24, 25–29, 30-35, 35–39, 40–44, and >45 years.
Frequency and percentage of the age are higher in the age range of 30-34 years, while the age range of >45 years is lower.
Figure 1 shows the distribution of pathological conditions by age, from which we note that the age group is 30–34 years. The highest was 40%, followed by the age group (25–29 years) with 35%. While the age group (over 45 years) was 10% lower, It shows the interest of middle-aged women to look for the ideal weight and treat obesity, unlike the elderly.
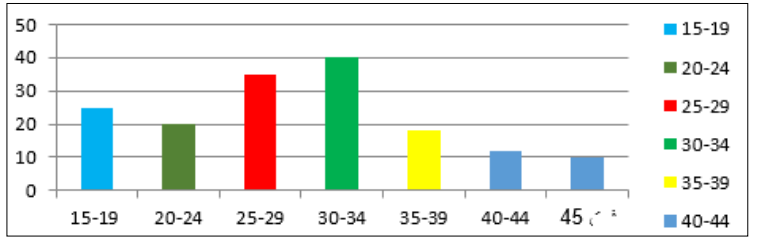
Figure 1: Distribution of Sick Cases by Age
Figure 2 shows the distribution of obesity patients according to their marital status, from which we note that the majority are married (53%). Followed by female bachelors (32%), and widows (15%), attributing this to the interest of married and single women in health and maintaining the ideal weight of their bodies.
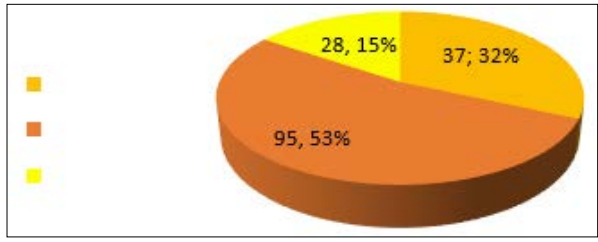
Figure 2: Distribution of Patients by Marital Status
Figure 3 shows the change in weight for the sample of the study, from which we observe the reduction in weight following diet number one for 132 (75%). Which depends on reducing the intake of starches and animal fats and replacing them with white meat and vegetable oils, fruits and vegetables, and half-hour walking.
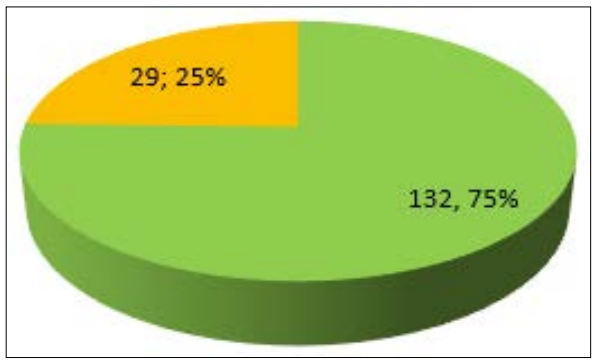
Figure 3: Weight Change Following Diet No. 1
Figure 4 shows the change in the quantity of triglycerides, from which we note the low level of triglycerides for 145 (91). This underscores the importance of Diet No. 1 in reducing triglycerides in the blood for the pathological conditions that followed this system and met its daily meal deadlines of 160 mg/dL. If there is no additional source of risk, 130 mg/dL in the case of angina, 100 mg/dL in the case of angina, and a second hazardous source, such as high blood pressure, stress, or smoking, 70 mg/dL in the case of several sources of hazards as described above in addition to diabetes, and the general public can reduce bad cholesterol by eating a teaspoon of fish oil daily. There are also capsules containing fish oil in the markets, in which case one capsule is taken every day. Fish oil (preferably North Atlantic fish type) contains good cholesterol, which the human body cannot manufacture. On the one hand, the body benefits from the advantages of good cholesterol. On the other hand, good cholesterol collects bad cholesterol from the blood and transfuses it to the liver for disposal. A spoonful of apple cider vinegar can also be added to the food so that the bad cholesterol in the blood decreases and its bad effect on arteries in general and heart arteries is reduced by the healthcare team.
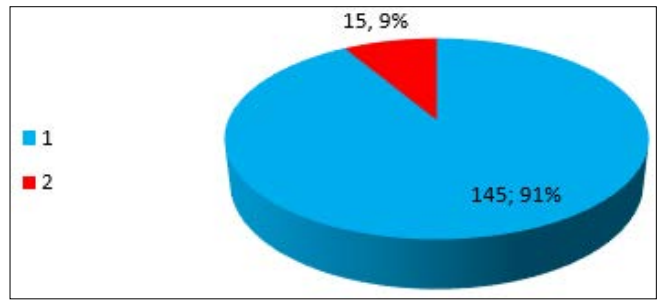
Figure 4: Triple Fat Change Following Diet No. 1
Figure 5 shows the change in the amount of cholesterol in the blood for patients in the study sample, from which we note the reduction of cholesterol in the blood for 125 (80%) patients. This represents a high percentage of the study sample, underscoring the importance of dieting 1 for weight loss and blood cholesterol reduction.
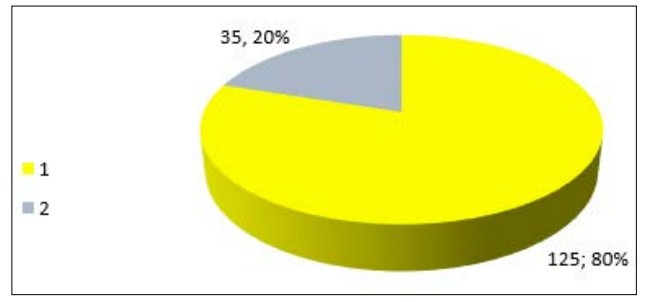
Figure 5: Cholesterol Change Following Diet No. 1
Figure 6 shows the weight change of the study sample individuals, through which we observe the low weight following diet 2 for 102 (58%). Despite exercising, the rate of low weight was lower than with diet No. 1. This underscores the importance of reducing starches, sweets, and red meat in any weight loss diet, especially for females.
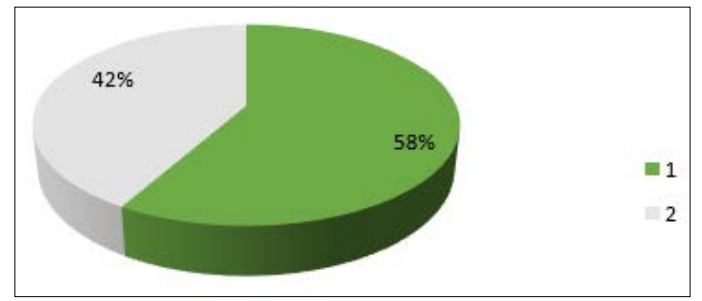
Figure 6: Weight Change Following Diet No. 2
Figure 7 shows a small reduction in weight and triglycerides to the normal level in 120 patients (77%). It is a high percentage, which confirms the success of this system in lowering triglycerides without any effect on cholesterol or the weight of the study sample individuals.
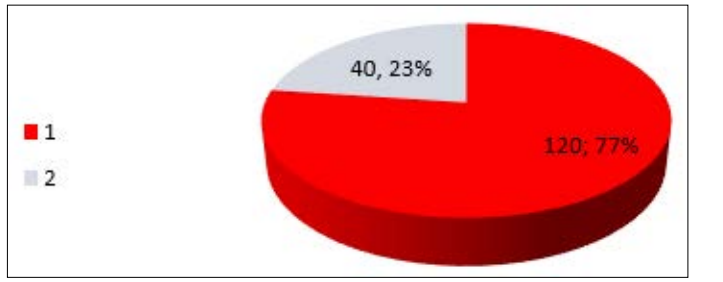
Figure 7:Triple Fat Change Following Diet No. 2
Figure 8 shows low blood cholesterol for study sample individuals where the blood cholesterol level decreased below the normal level of 120 patients (69%), which is high compared to the impact on weight despite the lack of interest in simple exercise such as walking.
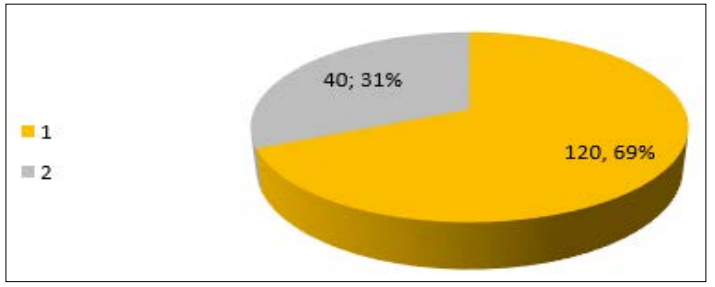
Figure 8: Cholesterol Change following Diet No. 2
Figure 9 shows the low weight following Diet No. 2, where the weight decreased following Order No. 3 for 27 (15%) patients. This is a very low percentage that expresses its inability to lose weight because it depends on high calories that are close to what the average person eats at home despite doing some exercises.
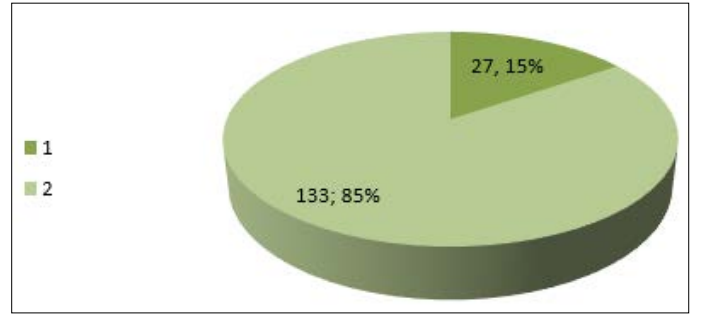
Figure 9: Weight Change Following Diet No. 3
Figure 10 shows the importance of following diet No. 2 in melting fat around the waist, as the decrease in waist circumference was good for 134 (85%) patients, despite the lack of use of physiotherapy and ultrasound.
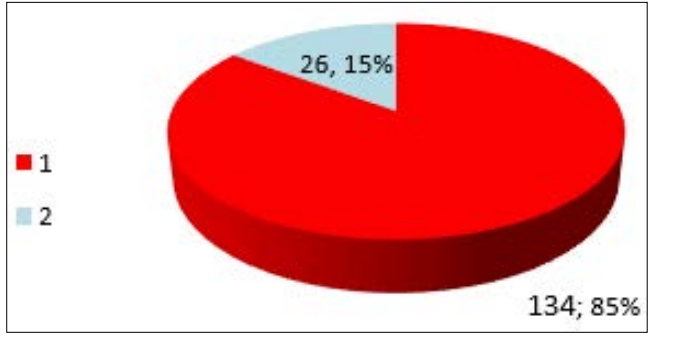
Figure 10: Change in waist circumference of patients following diet No. 2
Figure 11 shows the effectiveness of diet No. 2 in reducing weight, and the cholesterol level decreased for 98 (56%) patients. This is low due to a lack of exercise and not taking cholesterol fragmentation drugs recommended by doctors. Diet and exercise are the best ways to treat high low-density lipoprotein (LDL) levels in blood cholesterol.
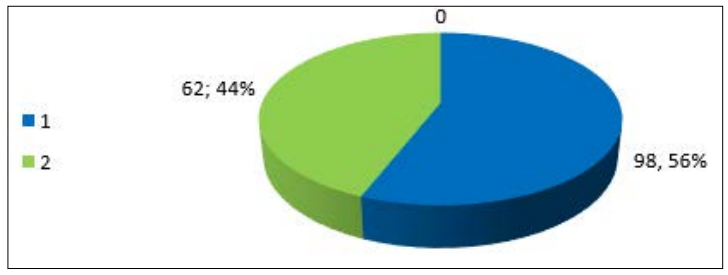
Figure 11: Change in cholesterol Diet No. 2
Risk factors for coronary artery disease include elevated levels of blood total cholesterol and LDL cholesterol [29,30]. Studies investigated into the nutritional condition of vegetarians in both white and black America. These authors found that vegetarians had lower levels of serum total and low-density lipoprotein (LDL), as well as cholesterol, and they hypothesized that vegetarians also had lower cardiovascular risk factors, i.e., lower blood pressure (BP) [31]. Which in similar to present study, we observed that consumption of fruit and vegetables is highly associated with prevention and a low risk of obesity, high blood fat, cholesterol, and cardiovascular disease.
The health benefits of two dietary patterns, the Mediterranean and Japanese ones, in which the consumption of plant foods has a significant place in both, may also be used to infer the positive function of fruit and vegetable consumption [32].
According to a another study [33,34]. African fruits and vegetables are abundant in dietary fiber, which has been linked to hypotensive and hypocholesterolemic effects. In addition, it has been demonstrated that the plant sterols prolong platelet aggregation following collagen epinephrine activation and lower plasma levels of low-density lipoprotein cholesterol [33].
Similar findings have been found in a study conducted by Gebharch, which suggests that the suppression of hepatic cholesterol production may be the cause of 900 effects of garlic [35,36].
This study indicates that consumption of three to five portions/day of fruit and vegetables is highly associated with prevention and a low risk of obesity, high blood fat, cholesterol, and cardiovascular disease. These findings support public health recommendations that people are at risk of developing obesity, blood fat, and cardiovascular disease; they need to eat more fruit and vegetables for more than the nine rations/day recommended by international organizations, which requires further research.
A healthy diet that helps prevent malnutrition includes: always including fruit and vegetables in meals in the season; replacing milk and its whole derivatives with low-fat or fat-free ones; replacing white bread with slow-absorbing brown bread, which gives a sense of satiety; Reduce the saturated fat ratio to less than 10% of total energy intake; eat more vegetables and fruits (at least 400 g) to reduce weight and blood fat; Eat whole foods instead of refined foods free of minerals and vitamins; eat white meat such as fish and poultry free of animal fat; educate children, adolescents, and adults about nutrition and healthy dietary practices. Educate children, adolescents, and adults about nutrition and healthy dietary practices. Strengthen fruit and vegetable drawers in school canteens to increase children’s consumption. Increase incentives that encourage producers and retailers to grow, use, and sell them. Review of therapeutic nutritionists to treat the risks of chronic non- communicable diseases. Develop standards to promote healthy dietary practices by ensuring the availability of healthy, nutritious, and safe food. Fruit and vegetables must be washed, peeled, and possibly cooked before eating them.
We thank the staff at Aspitar Hospital in Misrata City for permitting the study, particularly the therapeutic nutrition clinic staff.