Author(s): Selma Benkirane*, Zakia Douhi, Aida Oulehri, Hanane Bay Bay, Sara Elloudi and Fatima Zahra Mernissi
Pasini and Pierini’s atrophoderma is a rare dermatosis. The typical presentation is an ovoid lesion, slightly depressed, hyperpigmented of the trunk, occurring preferentially in the female sex [1-3]. We report a clinical particular aspect occurring in a young boy in the lower limbs.
Pasini and Pierini’s atrophoderma is a rare dermatosis. The typical presentation is an ovoid lesion, slightly depressed, hyperpigmented of the trunk, occurring preferentially in the female sex [1-3]. We report a clinical particular aspect occurring in a young boy in the lower limbs.
13-year-old patient, with no notable pathological history, referred in our training to complete the management of a vitiligo, presenting for 05 years hypochromic lesions of the asymptomatic lower limbs progressively increasing in size, then appearance of two other lesions in relation to shoulder blades with dermatological examination the presence of achromic macules of variable size, the largest of which is poorly defined 4cm with irregular border on the anterior (Figure 1 a) and posterior (Figure 1b) legs with depilation at the lesions, with a sign of positive traction, it there was no atrophy or sweating disorder or sensitivity, with two achromic plates well limited opposite the two shoulder blades (Figure 2). Wood light examination did not show any enhancement contrast [Figure 3]. Histology thus confirmed the diagnosis of atrophodermal type morphology of Pasini and Pierini by showing an atrophy of the epidermis with hyperpigmentation of the base, a peri-vascular lymphocytic infiltrate and a discrete anomaly of cutaneous collagen in focal edematous fibers and slightly homogenized, the skin appendices were preserved. Calcipotriol “DAIVOBET” was offered to the patient for the first time because he could not afford the topical calcineurin inhibitor “TACROLIMUS”, the evolution was marked by a total regression of lesions after 6 months (Figure 4)
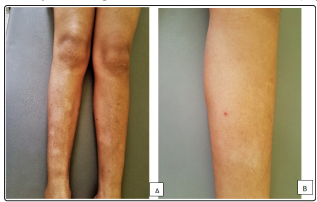
Figure 1: Clinically, the presence of achromic macules of variable size, the largest of which is poorly defined 4cm with an irregular border on the anterior (A) and posterior (B) legs with depilation at the level lesions

Figure 2: Presence of two achromic plates well limited opposite the two shoulder blades

Figure 3: Wood light examination did not show any enhancement contrast.

Figure 4: A total regression of lesions after 6 months
Pasini and Pierini’s atrophoderma is a rare disease, exclusively cutaneous, whose etiopathogenesis remains subject to controversy, it was initially described by Pasini in 1923 and Pierini in 1936, occurs most often in women, with a peak of incidence in the second and third decades of life [4]. Congenital cases have been described. The pathophysiology of this entity remains unknown and the role of Borrelia burgdorferi infections remains controversial [5]. It was included as a manifestation of localized scleroderma in the superficial form of multiple forms. It is characterized clinically by very few sclerotic and sometimes atrophic plaques, they are typically immediately pigmented, hypopigmented in certain cases, or colored Normal skin.
They predominate on the trunk and the ends. The evolution is slow over several years, spontaneous regressions are described with persistence, most often pigmentation [6]. On histopathological examination, the epidermis is generally normal or slightly atrophic. Melanin is increased in the basal layer, and interstitial edema and a slight perivascular infiltrate, composed of lymphocytes and histiocytes, may be present. Collagen bundles exhibit different degrees of homogenization and discharge in the median and reticular dermis, with a normal papillary dermis. The skin appendices are preserved [7,8]. No treatment is consistently effective for Pasini and Pierini’s atrophodermia, but some patients respond to topical corticosteroids, antibiotics, synthetic antimalarials, phototherapy, and Q-switched Alexandrite laser has also been reported, leading to improvement clinic of hyperpigmented lesions.
Pasini and Pierini atrophodermia should be sought before hypopigmented lesions in the lower limbs. An anatomopathological examination is a key step which supports the diagnosis.